
Vitamin D is a major and easily modifiable factor that helps reduce the incidence and severity of COVID-19.
 Many studies to date have demonstrated a reduced risk of COVID-19 infection, severity, and death with increased vitamin D levels, as well as with other important nutrients.
Many studies to date have demonstrated a reduced risk of COVID-19 infection, severity, and death with increased vitamin D levels, as well as with other important nutrients.
 Many studies to date have demonstrated a reduced risk of COVID-19 infection, severity, and death with increased vitamin D levels, as well as with other important nutrients.
Many studies to date have demonstrated a reduced risk of COVID-19 infection, severity, and death with increased vitamin D levels, as well as with other important nutrients.The eBook, Vitamin D & COVID-19, A Summary of Published Research, is a condensed and concise compilation of much of the published research on vitamin D and COVID-19, easy to read and share as a downloadable, printable PDF. Your purchase helps to further public knowledge and education of this invaluable research!
Purchase Vitamin D & COVID-19 eBook
Below we present up-to-date scientific information on the following topics:
COVID-19 and Vitamin D – Study Results
Infection – Severity & Death – Recovery
COVID-19 and Other Nutrients – Study Results
Immune Function & Co-Nutrients
Flu, Colds & Other Respiratory Infections
COVID-19 and Vitamin D – Study Results
Another Vitamin D and COVID-19 Meta-Analysis, with Similar Conclusions
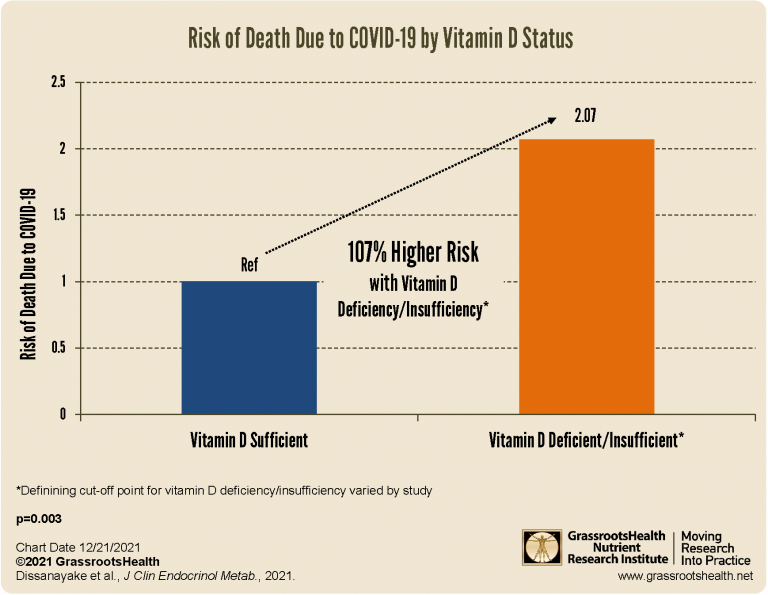
A total of 72 studies with data from 1,976,099 individuals was included in the meta-analysis by Dissanayake et al.. The study found that those with vitamin D deficiency/insufficiency had a
- 46% higher risk of developing COVID-19
- 90% higher risk of developing severe COVID-19 disease
- and a 107% higher risk of death due to COVID-19
![]()
Meta-Analysis: Demonstrated Effectiveness of Vitamin D for COVID-19
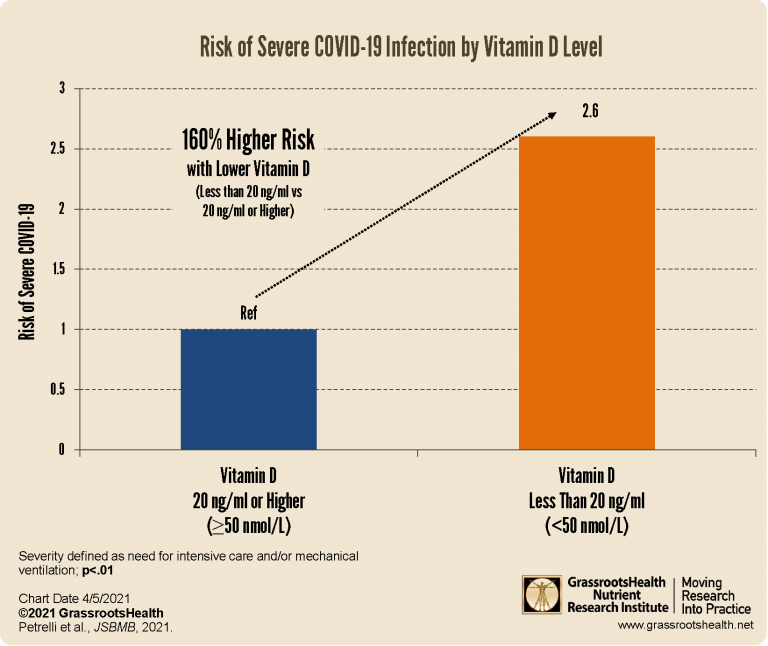
A review by Petrelli et al. included 43 studies with data from a total of 612,601 COVID-19 patients that had been published from the beginning of the COVID-19 pandemic through January 31, 2021. COVID-19 disease risk, severity, and/or mortality was assessed among individuals with or without vitamin D deficiency (defined as vitamin D levels below 20 ng/ml or 50 nmol/L).
- Risk of COVID-19 infection was 50% higher among those whose vitamin D levels were below 20 ng/ml
- Risk of severe COVID-19, defined as the need for intensive care and/or mechanical ventilation, was 160% higher among those with vitamin D levels below 20 ng/ml
- Risk of death due to COVID-19 was 22% higher among those with vitamin D levels below 20 ng/ml
- Vitamin D supplementation of various doses reduced the risk of severe COVID-19 disease by 73% and death by 59%
![]()
Analysis Shows Potential for Zero COVID-19 Deaths at 50 ng/ml or Higher Vitamin D
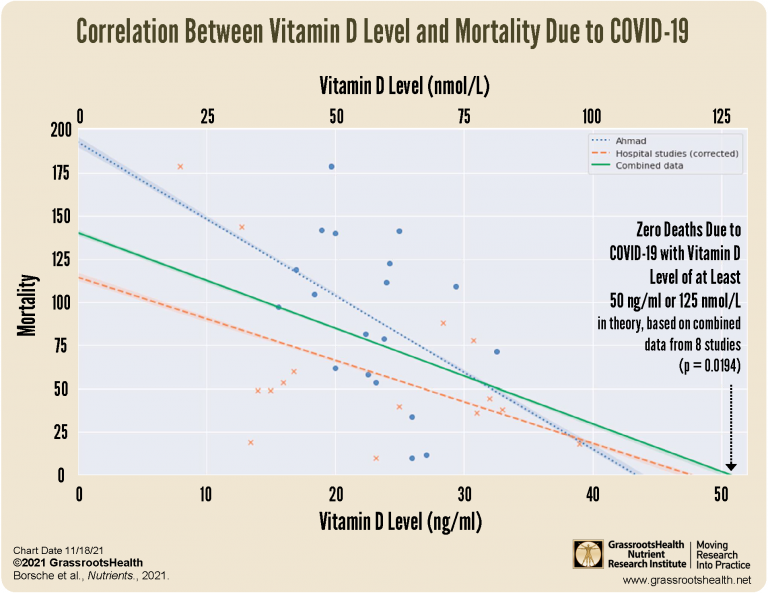
A systematic review by Borsche et al. used data from 8 studies to determine a potential optimal vitamin D level to minimize COVID-19 mortality. The study confirmed an inverse correlation between COVID-19 mortality and vitamin D levels, which showed that as vitamin D levels increase, COVID-19 mortality decreases, to a point where the projected mortality rate reaches zero at a vitamin D level of around 50 ng/ml (125 nmol/L). This paper reviews how
- Vitamin D deficiency limits immune system performance, increases the spread of diseases, reduces protection against infections, reduces effectiveness of vaccination, and is a main cause of severe COVID-19 illness
- Vitamin D status correlates with length of ongoing COVID disease, severity of symptoms, and mortality risk
![]()
COVID-19 Infection
New Study Shows ~50% Lower COVID-19 Positivity Rate among those with Higher Vitamin D Levels
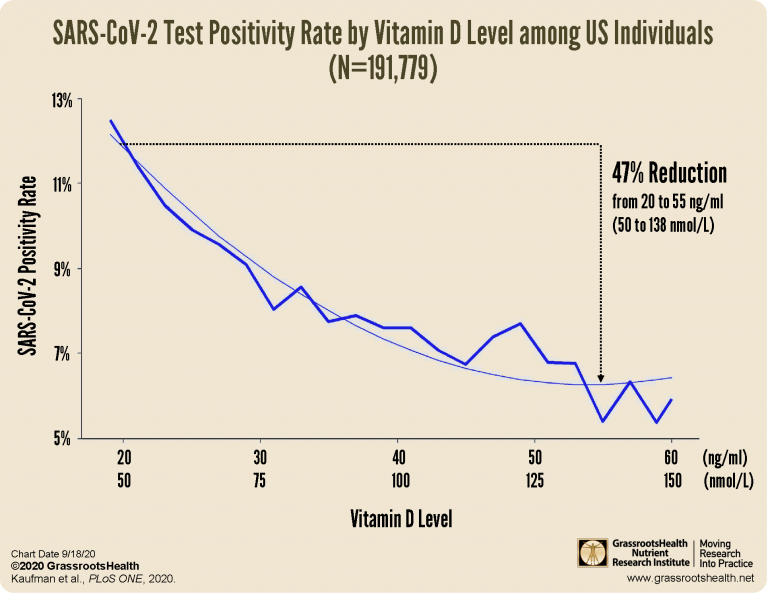
A paper by Kaufman et al. (including our own Scientists Panel member Dr. Michael F. Holick) looked at vitamin D levels over the past year and COVID-19 test results from March to June of 2020. Data from over 190,000 patients from 50 states who were tested at Quest Diagnostics lab were included. The investigators used zip code data to match with US Census data to perform analyses based on race/ethnicity and latitude. The researchers found that the percent of positive SARS-CoV-2 tests was 12.5% for those with vitamin D levels less than 20 ng/ml (50 nmol/L) and 5.9% for those with levels at or above 55 ng/ml (138 nmol/L), which is a 53% lower positivity rate with higher vitamin D levels!
![]()
Vitamin D Level Below 30 ng/ml (75 nmol/L) an Independent Risk Factor for COVID-19
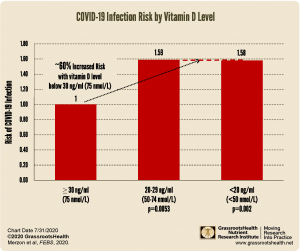
Merzon et al. examined data from individuals in Israel who were tested for COVID-19 infection between February 1st and April 30th of 2020 to see if there was an association between low vitamin D levels and the risk of COVID-19 infection and hospitalization. The data showed an almost 60% increased risk in COVID-19 infection for individuals whose vitamin D level was below 30 ng/ml (75 nmol/L) compared to individuals whose vitamin D level was 30 ng/ml or higher. The analysis also found that among the COVID-19 positive individuals, there was an almost doubled risk of hospitalization for those whose vitamin D levels were below 30 ng/ml.
![]()
VIDEO: If Vitamin D is Less than 20 ng/ml (50 nmol/L), 77% More Likely to Test Positive for COVID-19

In this video, Dr. Ian Smith of the show The Doctors interviews Dr. David Meltzer from the University of Chicago about the findings of his recent study, which found that patients who had tested vitamin D deficient (less than 20 ng/ml or 50 nmol/L) were about 77% more likely to test positive for COVID-19 than patients whose vitamin D level was not deficient.
![]()
COVID-19 Severity & Death
14 Times Higher Risk of Severe or Critical COVID-19 Disease with Pre-Infection Vitamin D below 20 ng/ml (50 nmol/L)

A study by Dror et al. looked at pre-infection vitamin D levels among 253 patients hospitalized with COVID-19, and compared those levels to COVID-19 disease severity. The study found that 57% of those with pre-infection vitamin D levels below 20 ng/ml ended up with severe or critical COVID-19, severe or critical COVID-19 was 87% less likely among patients whose pre-infection vitamin D level was at least 40 ng/ml compared to below 20 ng/ml, and patients with pre-infection vitamin D levels below 20 ng/ml were 14 times more likely to have severe/critical COVID-19 compared to those at or above 40 ng/ml. Further analysis found the strongest correlation between vitamin D level and COVID-19 disease severity among those who were 50 years or older.
![]()
Study Concludes Vitamin D Treatment Reduces COVID-19 Deaths
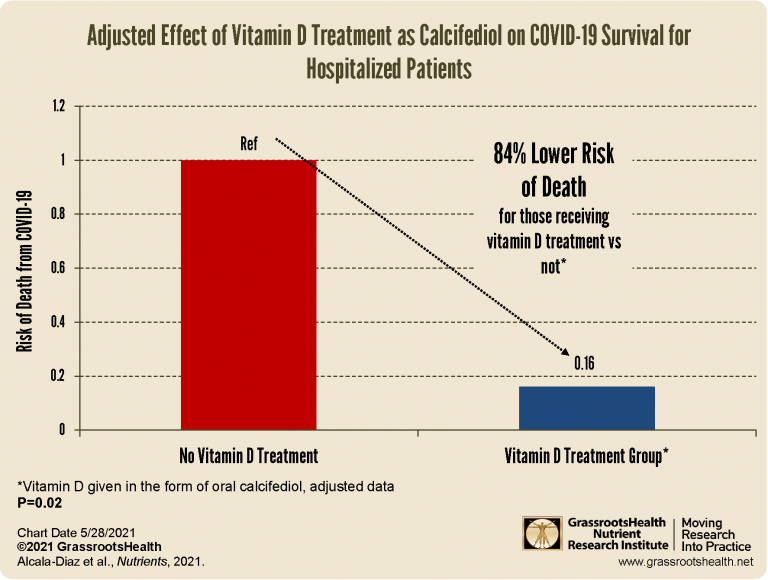
A study published by Alcala‐Diaz et al. looked at the mortality rate during the first 30 days after admission of patients receiving vitamin D treatment (in the form of calcifediol) in combination with the standard of care, compared to patients receiving only the standard of care. Unadjusted data showed the mortality rate among those receiving the vitamin D treatment was 5% compared to a mortality rate of 20% among those not receiving vitamin D (OR=0.22, P<0.01); a 78% lower risk of death for those receiving vitamin D treatment vs not. The adjusted data showed an 84% reduced risk of death for those receiving vitamin D treatment vs not (P=0.02), which is a more precise indicator of the relationship between the risk of death from COVID-19 and the vitamin D treatment itself.
![]()
Vitamin D Treatment for COVID-19 Patients Nearly Erased Need for ICU Admission
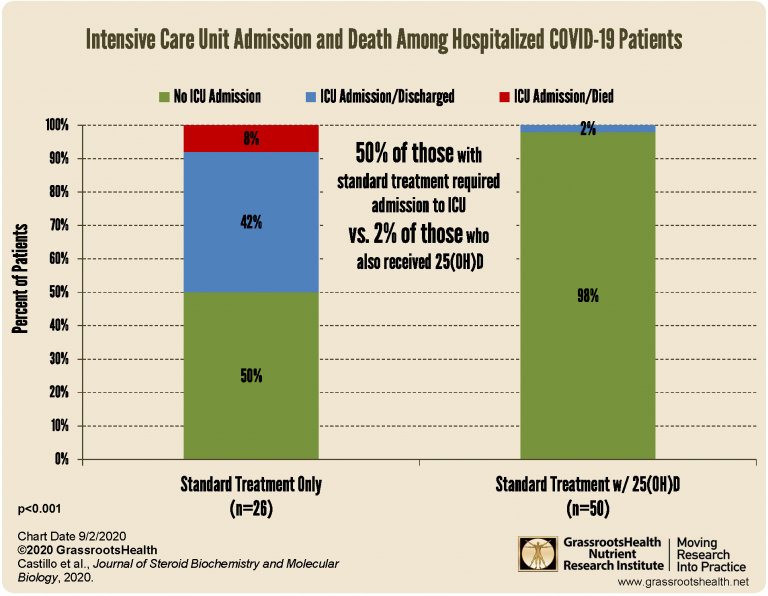
One of the latest studies on vitamin D and COVID-19, published by Castillo et al., enrolled 76 COVID-19 patients hospitalized with symptoms of acute respiratory infection and randomized them to the vitamin D treatment group (n=50) or the control group (n=26). There were 45 men and 31 women with an average age of 53 years. Their goal was to determine if early intervention with 25(OH)D, the metabolite of vitamin D used to measure vitamin D status, could improve outcomes of COVID-19 and reduce the need for Intensive Care Unit (ICU) admission. Of the 26 patients in the control group, 13 (50%) required admission to the ICU with two resulting deaths, while only one patient out of the 50 (2%) in the vitamin D group required admission to the ICU, with no resulting deaths.
![]()
15 Fold Higher Risk of Death due to COVID-19 with Vitamin D <12 ng/ml
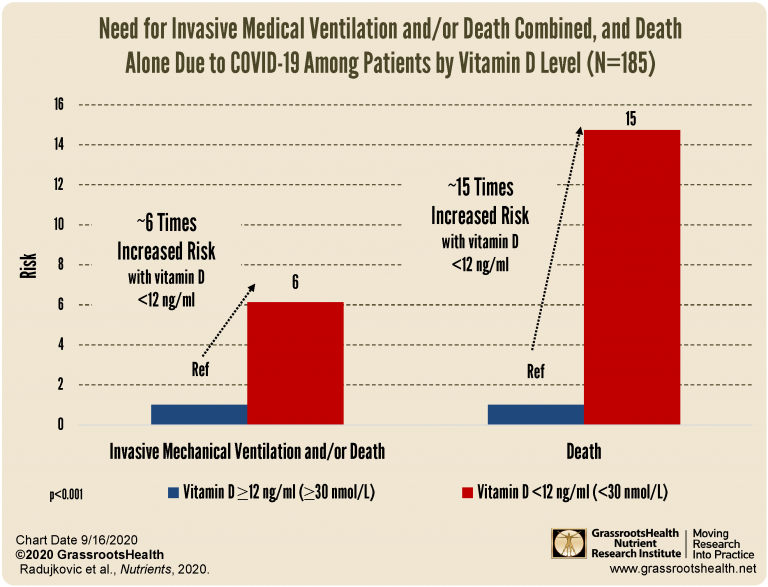
A study by Radujkovic et al. analyzed data from 185 COVID-19 patients to see if vitamin D status at hospital admission had any association with COVID-19 disease severity and survival. Patients admitted for inpatient care were more likely to have a vitamin D level below 12 ng/ml (30 nmol/L). By the end of the study, a total of 16 patients had died, and 23 patients required invasive mechanical ventilation. Those with a vitamin D level below 12 ng/ml had a 6-fold higher risk of severe disease resulting in the need for invasive mechanical ventilation and/or death, and approximately 15 fold higher risk of death.
![]()
Another Study Matches COVID-19 Disease Severity and Death to Vitamin D Levels
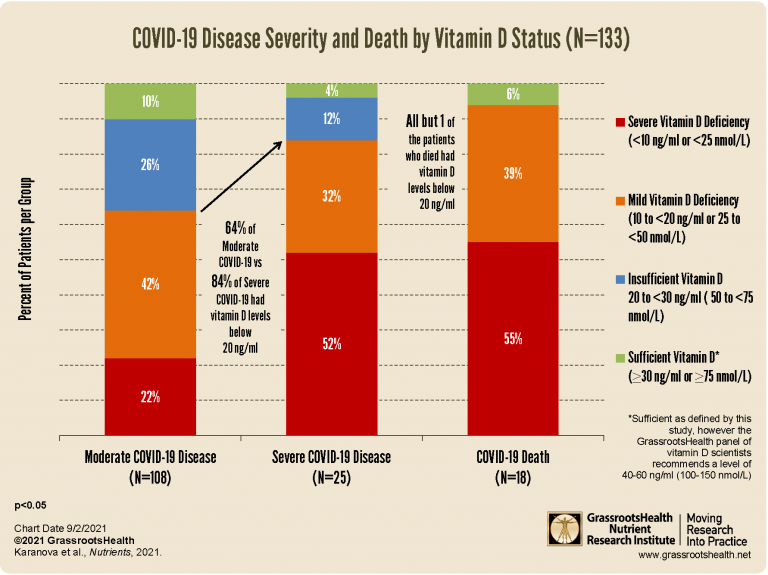
A study by Karanova et al. found a significant relationship between low vitamin D levels and severity and death among patients hospitalized with COVID-19. This study included 133 patients whose vitamin D levels at hospital admission ranged from 3 ng/ml to 97 ng/ml. 81% of the patients had a moderate course of disease. Of those suffering a severe course of COVID-19, 35% were severely vitamin D deficient and 15% were mildly vitamin D deficient. Only one of the 18 patients (6%) who died from COVID-19 had a vitamin D level greater than 20 ng/ml (50 nmol/L). This study concluded that disease severity and death due to COVID-19 were both associated with vitamin D deficiency (levels below 20 ng/ml or 50 nmol/L), with increased significance among those whose vitamin D level was severely deficient, below 10 ng/ml (25 nmol/L). Those with vitamin D levels less than 10 ng/ml had more than 4 times the risk of severe disease and almost 6 times the risk of dying from COVID-19 compared to those 10 ng/ml and higher.
![]()
Higher Chance of Being Hospitalized with COVID-19 if Vitamin D Deficient
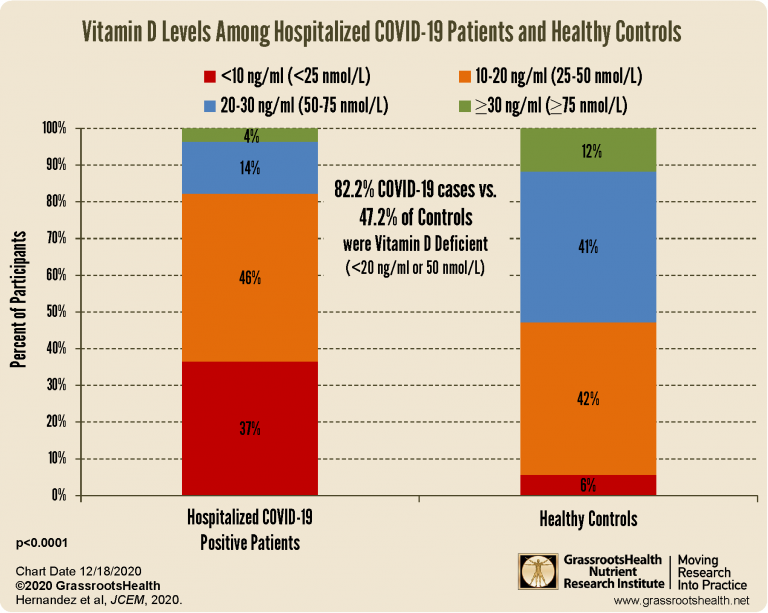
A study by Hernandez et al. looked at vitamin D levels among 216 adult hospitalized COVID-19 patients and compared them to levels of 197 matched healthy controls. The average vitamin D level among the COVID-19 patients upon admission to the hospital was 14 ng/ml (35 nmol/L) with 82% having vitamin D levels below 20 ng/ml (50 nmol/L), and an average of 21 ng/ml (52 nmol/L) among healthy controls, with only 47% below 20 ng/ml (p<0.0001). Also, the patients with higher vitamin D levels had better PaO2/FIO2 ratios, less frequent radiological progression, were less likely to require medication or be admitted to the ICU, and were more likely to have a shorter hospital stay.
![]()
Re-Confirmed: Vitamin D Deficiency is a Risk Factor for COVID-19 Disease Severity
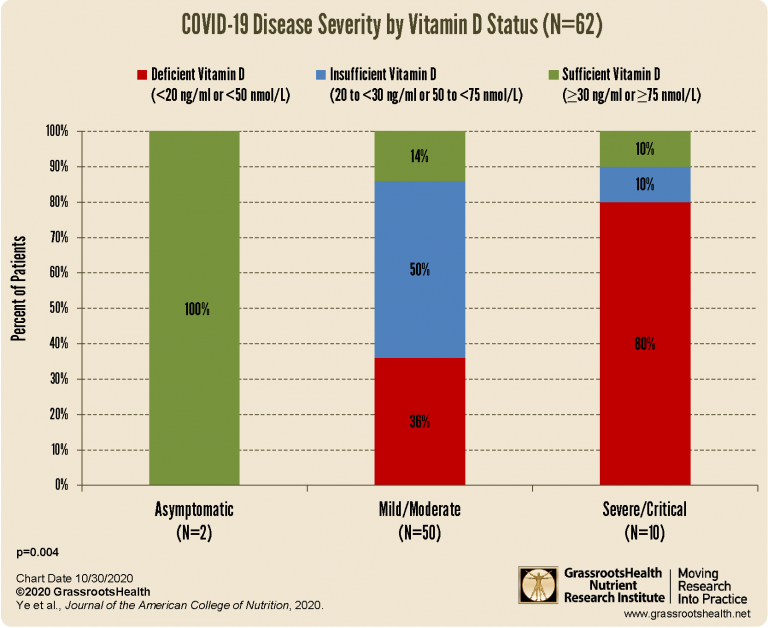
In a case-controlled study, Ye et al. compared vitamin D levels of 80 healthy controls to those of 62 hospitalized COVID-19 patients to determine if there was a relationship between vitamin D level and COVID-19 infection and severity. Among COVID-19 positive patients 42% were vitamin D deficient and the average level was 22.3 ng/ml (55.6 nmol/L), compared to 19% deficient and an average level of 28.8 ng/ml (71.8 nmol/L) among healthy controls. Patients with severe/critical COVID-19 cases were more likely to be older, have comorbidities, and have lower vitamin D levels than patients with mild/moderate cases.
![]()
Increased Mortality Rate among COVID-19 ARDS Patients with Severe Vitamin D Deficiency
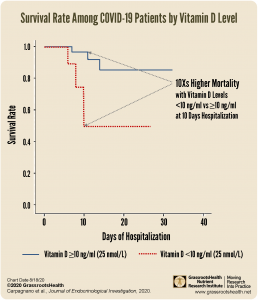
A study published by Carpagnano et al. looked at data from 42 hospitalized patients in Italy who had been diagnosed with acute respiratory failure due to COVID-19. 81% of the patients with acute respiratory failure due to COVID-19 had vitamin D levels below 30 ng/ml (75 nmol/L); and 24% had severe vitamin D deficiency (≤10 ng/ml or ≤25 nmol/L). When looking at mortality rates after 10 days of hospitalization, it was found that those with severe vitamin D deficiency had a 50% probability of death, compared to 5% among those with a vitamin D level greater than 10 ng/ml (25 nmol/L).
![]()
COVID-19 Patients in ICU at Higher Risk of Death if Vitamin D Deficient
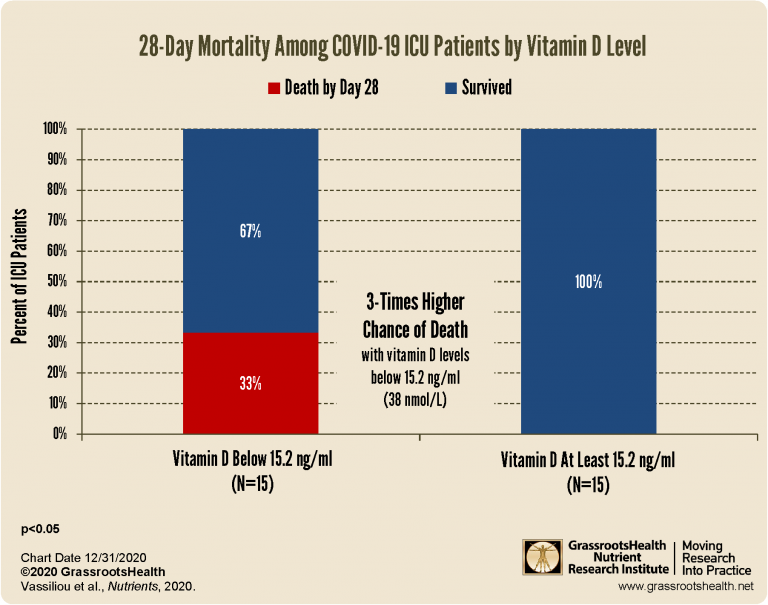
In a prospective, observational study, Vassilious and colleagues investigated COVID-19 patients who were admitted to the ICU to see whether low vitamin D levels put them at greater risk of mortality. Critically ill patients diagnosed with COVID-19 pneumonia who were admitted to the ICU of a Greek hospital had their vitamin D levels measured. By 28 days, five of the patients with vitamin D levels below 15.2 ng/ml died whereas none of the patients in the group with a vitamin D level of at least 15.2 ng/ml had died.
![]()
Higher Vitamin D Status Associated with Better Clinical Outcomes in Patients Hospitalized with COVID-19
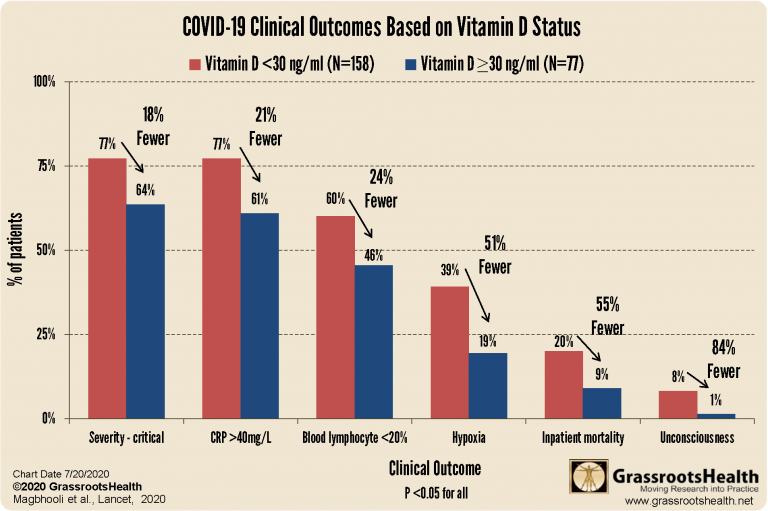
Maghbooli et al. present the results from a study in which they analyzed hospital medical records from patients hospitalized with COVID-19 (part of their COVID-19 prospective patient registry). They found that vitamin D levels over 30 ng/ml (75 nmol/L) were associated with better clinical outcomes. The authors further analyzed the data based on vitamin D blood levels of at least 40 ng/ml (GrassrootsHealth’s Scientists’ Panel recommends a level between 40-60 ng/ml (100-150 nmol/L)). Although there were not enough patients for a full analysis based on this classification, they found that of those over 40 years old with vitamin D blood levels less than 30 ng/ml, 20% died from COVID-19, whereas in those with blood levels of at least 30 ng/ml, 9.7% died, and in those with vitamin D levels of at least 40 ng/ml, 6.3% died.
![]()
Comparing Asymptomatic to Critically Ill COVID-19 Patients
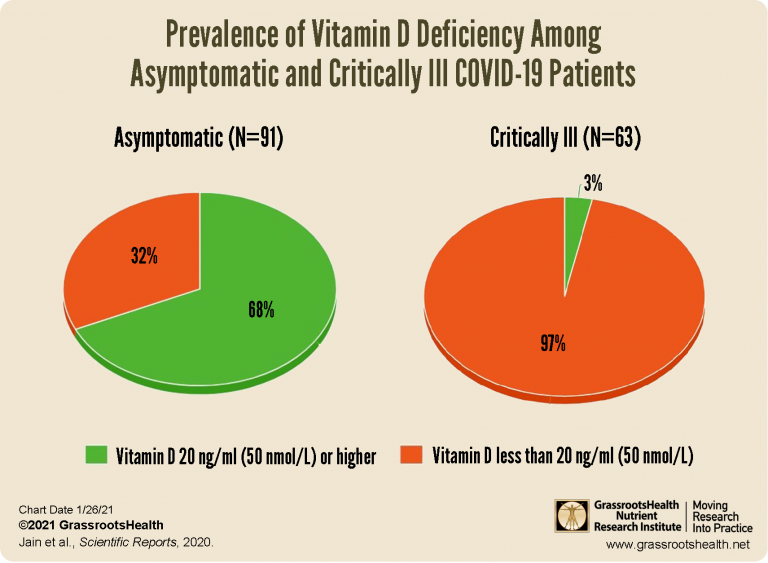
An observational study by Jain et al. looked at 154 patients positive for COVID-19, ages 30-60 years old, who were admitted to a tertiary COVID-19 care center over a span of 6 weeks in 2020. Of the patients, 91 were asymptomatic, displaying no symptoms over 12 days from testing positive. These patients were compared to 63 others who developed severe enough symptoms to require admission to the Intensive Care Unit (ICU). The average vitamin D level in the asymptomatic group was 28 ng/ml (70 nmol/L) with 29 patients (32%) having levels below 20 ng/ml or 50 nmol/L (labeled as being deficient). The average vitamin D level in the critically ill group was 14 ng/ml (35 nmol/L) with 61 (97%) below 20 ng/ml.
![]()
Reduced Death and Disease Severity with Vitamin D Supplementation Prior to COVID-19 Diagnosis
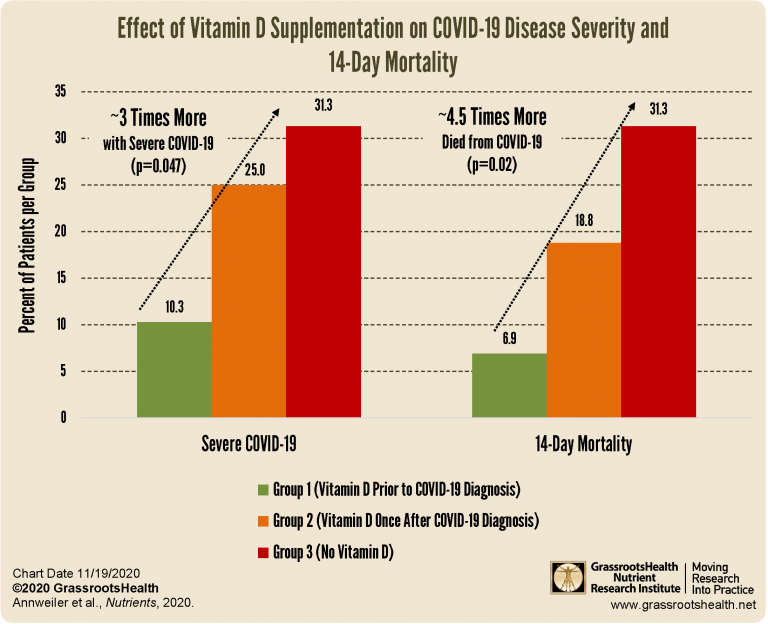
This study, by Annweiler et al., included data from 77 patients, age 78 to 100 years, consecutively hospitalized into a geriatric unit for COVID-19. The patients were assigned to one of three groups; Group 1 had regularly supplemented with bolus doses of vitamin D over the past year (either 50,000 IU per month or 80,000 or 100,000 IU every 2-3 months) and did not receive additional vitamin D after being diagnosed with COVID-19, Group 2 was given 80,000 IU vitamin D within a few hours after being diagnosed with COVID-19, and Group 3 did not have any vitamin D supplementation prior to or after diagnosis. The 14-day mortality was 31.3% among those in Group 3 compared to only 6.9% among those in Group 1, equating roughly to a 4.5 times greater mortality risk among those in Group 3. A similar association was seen for COVID-19 disease severity, with three times those in Group 3 (31.3%) experiencing severe symptoms compared to Group 1 (10.3%).
![]()
Children, COVID-19 & Vitamin D
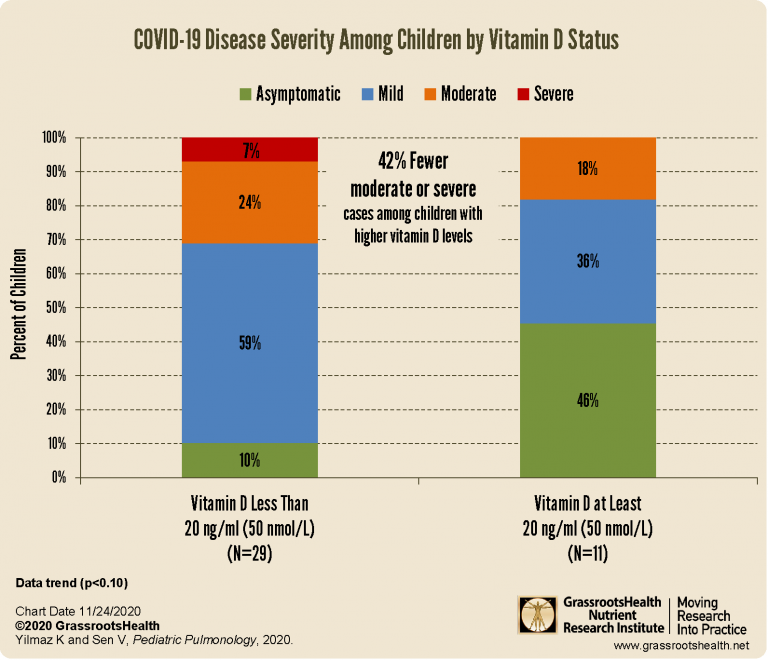
When disease severity for the children who were diagnosed with COVID-19 was analyzed according to vitamin D level, a trend was found showing increased disease severity for those with lower vitamin D levels. In fact, among those with a vitamin D level below 20 ng/ml (50 nmol/L), 31% of the children had moderate to severe COVID-19 symptoms, compared to only 18% with moderate symptoms (none classified as severe) for those children with vitamin D levels of 20 ng/ml or higher. Additionally, 46% of the children with higher vitamin D levels were asymptomatic, compared to 10% of those with lower vitamin D levels.
![]()
Factors Associated with COVID-19 Hospitalization and Disease Severity
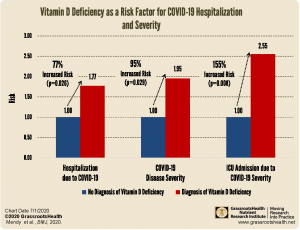
Mendy et al. looked at medical record data from 689 patients diagnosed with COVID-19 in the University of Cincinnati health system and analyzed it to identify potential risk factors associated with COVID-19 hospitalization (a hospital stay of at least 24 hours) and severity (defined as intensive care unit admission and/or death during hospitalization). Vitamin D deficiency significantly increased the risk of hospitalization due to COVID-19 (77% increased risk), COVID-19 disease severity (95% increased risk), and the need for intensive care unit admission due to COVID-19 (155% increased risk).
![]()
VIDEO: Can Vitamin D be Considered a Therapeutic Agent for COVID-19?
In this video, Professor Roger Seheult, MD explains the role vitamin D may have in the prevention and treatment of COVID-19. It contains excellent illustrations on how vitamin D works, summarizes the best available data and clinical trials on vitamin D, respiratory diseases, and COVID-19, discusses vitamin D dosage recommendations, and more.
![]()
COVID-19 Recovery
Vitamin D Shown to Increase Viral SARS-CoV-2 RNA Clearance
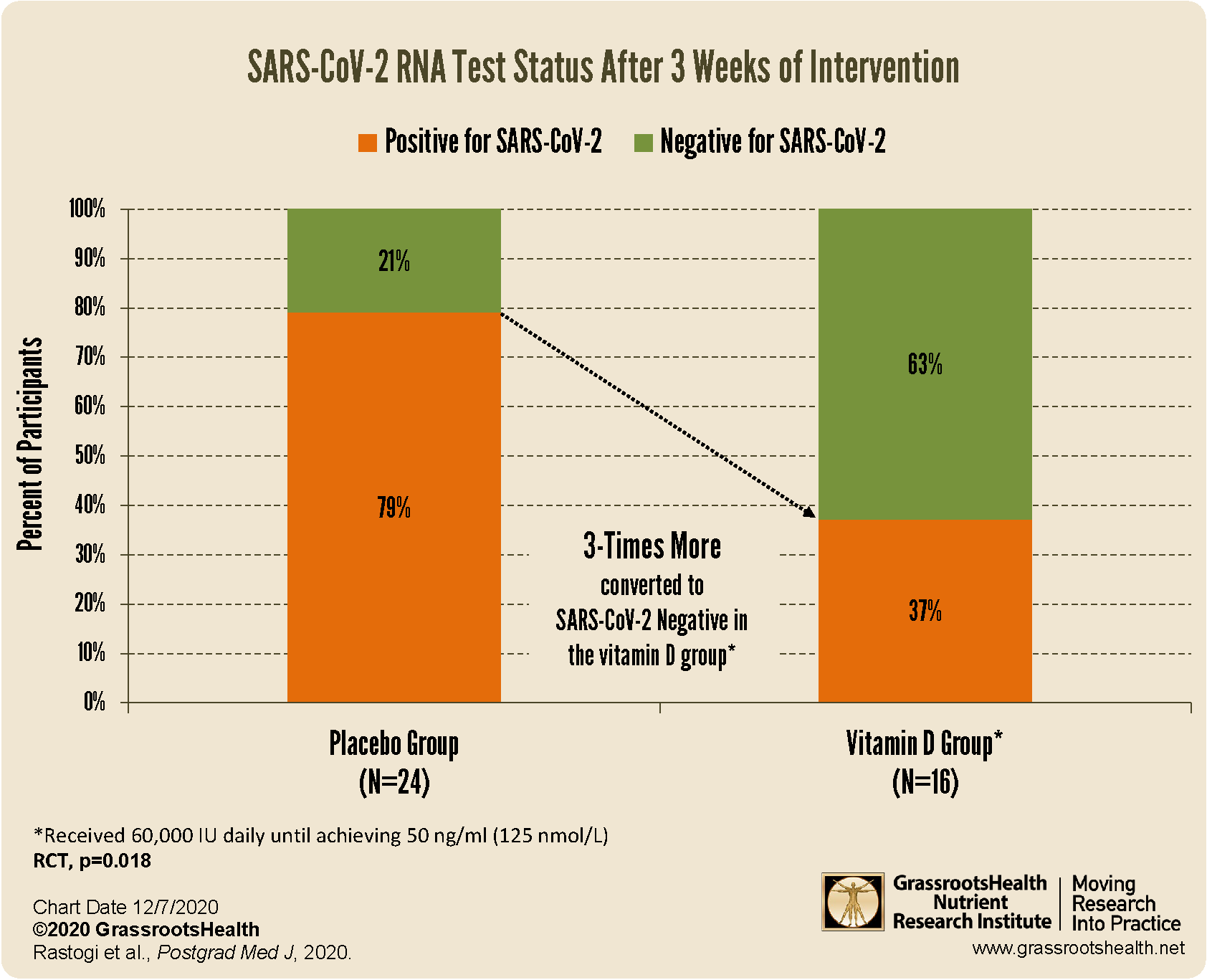
An RCT by Rastogi et al. randomized 40 patients who were hospitalized with a SARS-CoV-2 positive test and who were vitamin D deficient (with levels below 20 ng/ml or 50 nmol/L) into a study to determine if short-term, high-dose vitamin D supplementation with a target vitamin D level of 50 ng/ml (125 nmol/L) had an effect on SARS-CoV-2 test status. By the end of 3 weeks, ten of the 16 participants (63%) in the vitamin D group became SARS-CoV-2 negative, compared to only five of the 24 participants (21%) in the control group (p=0.018). Three times more participants in the vitamin D group converted from SARS-CoV-2 positive to negative after 3 weeks compared to those who did not receive any vitamin D. This strongly indicates that supplementing with vitamin D to reach a serum level of at least 50 ng/ml (125 nmol/L) among asymptomatic and mildly symptomatic SARS-CoV-2 positive individuals provides a much greater chance of testing negative compared to those who are vitamin D deficient.
![]()
Randomized Clinical Trial Shows Benefits of Vitamin D for COVID-19 Recovery
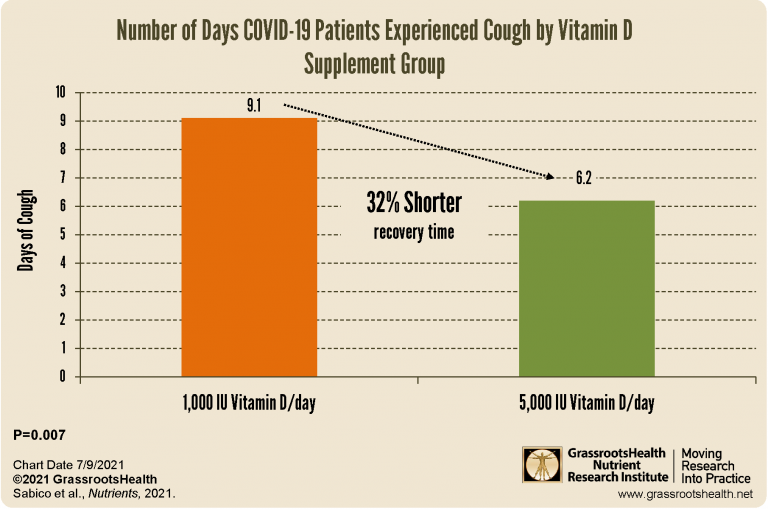
An RCT by Sabico et al. compared the effects of two weeks of supplementation with either 5000 IU vitamin D per day or 1000 IU vitamin D per day for individuals hospitalized with mild to moderate COVID-19. There was no significant difference in vitamin D levels between the groups at enrollment, however, after two weeks of supplementation, vitamin D levels significantly improved only among those taking 5000 IU vitamin D per day, increasing by 19% (p=0.003). Those taking 5000 IU per day also had a 32% shorter recovery time compared to those taking only 1000 IU per day in resolving cough (6.2 days compared to 9.1 days, p=0.039) and a 33% shorter recovery time for ageusia, or loss of taste (11.4 days compared to 16.9 days, p=0.035).
![]()
COVID-19 and Other Nutrients – Study Results
Nutritional Support Greatly Improves COVID-19 Outcomes with 86% Lower Mortality
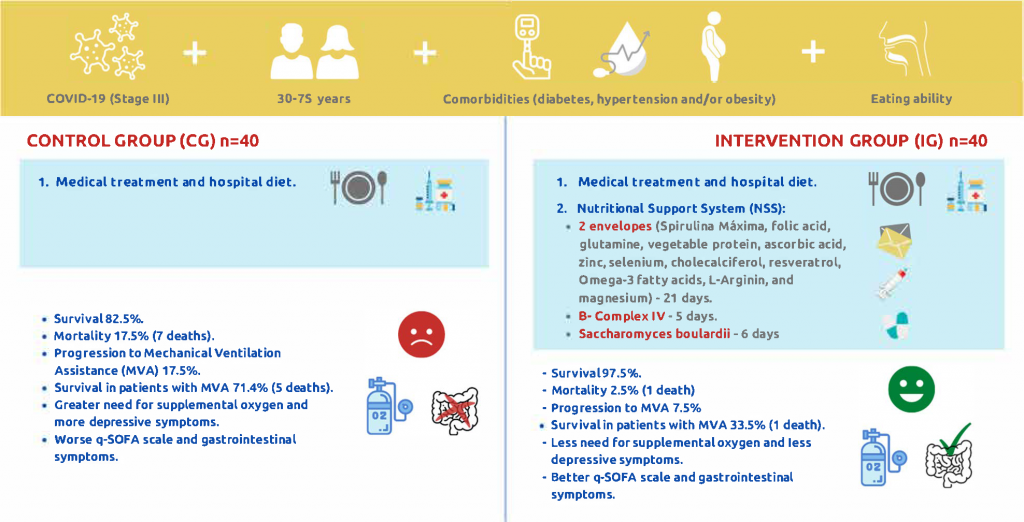
A randomized controlled clinical trial found that providing severe COVID-19 patients with nutritional support resulted in significantly increased survival rates; in fact, 7 times more patients died from COVID-19 without a nutritional support system compared to those who received nutritional support. The study also found that nutritional support resulted in decreased progression to mechanical ventilation, reduced intubation period, decreased need for supplemental oxygen, improved mood, and less occurrence of post-COVID syndrome.
![]()
Omega-3 Supplementation in Patients with COVID-19 Improves Chances of Survival by 7 Times
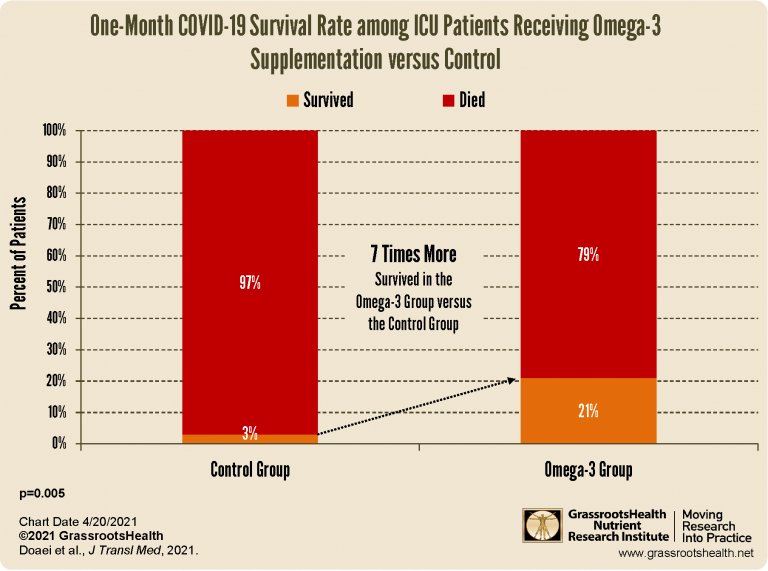
A double-blind, randomized controlled clinical trial by Doaei et al. looked at the effects of omega-3 fatty acid supplementation on inflammatory and biochemical markers among COVID-19 patients in the intensive care unit (ICU). When looking at the survival rate among both groups, those who were in the omega-3 supplement group had a significantly higher chance of survival at one month; a 21% chance of surviving for those treated with omega-3 supplements compared to only 3% survival for those not receiving omega-3s (p=0.005). That is a 7 times higher chance of surviving for those receiving omega-3 fatty acid supplementation.
![]()
Vitamin D and K Status Related to COVID-19 Disease Severity
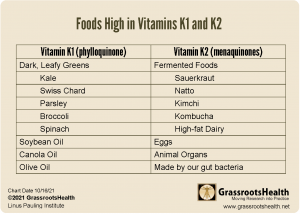
An observational study by Desai et al. looked at vitamin D and vitamin K status among 100 SARS CoV-2 positive patients whose COVID-19 disease presentation varied from asymptomatic to life-threatening and/or death and 50 age and sex matched healthy controls. Vitamin K status was worse (as indicated by higher dp-ucMGP levels) among COVID-19 positive individuals, and was also significantly and independently associated with chronic kidney disease, cardiovascular disease, hypertension, cancer/immunosuppression, and CRP. Decreased vitamin D levels were also significantly related to increased COVID-19 disease severity, with every 1-unit decrease in log vitamin D level associated with more than 3 times the likelihood of increased disease severity.
![]()
COVID Outcomes among Patients Receiving Vitamin D, Magnesium, and B12
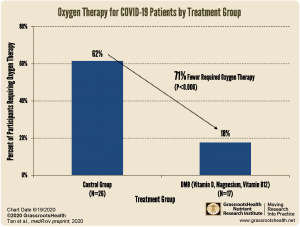
This study found that those receiving the DMB combination were significantly less likely to require subsequent oxygen therapy or intensive care support, meaning that simply taking vitamin D, magnesium and vitamin B12 supported immune and lung function. Only 3 out of the 17 patients (18%) in the DMB group required subsequent oxygen therapy, two of which required the therapy within 24 hours after their first supplement dose. For the patients who did not receive supplementation, 16 of the 26 (62%) required subsequent oxygen therapy. There was a significant protective effect against clinical deterioration with the need for oxygen therapy for DMB supplementation, after adjusting for age (P=0.039) or hypertension (P=0.044) separately.
![]()
Could Your Gut Bacteria Influence COVID-19 Outcomes and Vaccine Effectiveness?
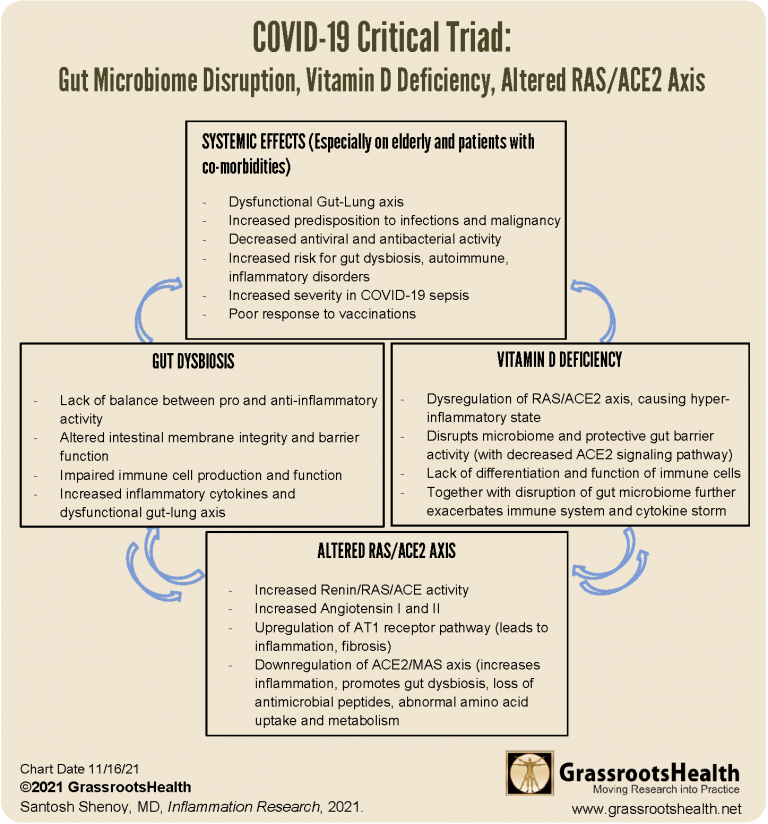
Dr. Santosh Shenoy, MD, of the University of Missouri, Kansas City Medical Center, investigated the published research to learn more about the connection between the gut microbiome, ACE-2 expression (an important factor controlling inflammation during SARS-CoV-2 infection), and vitamin D, in relation to severity of COVID-19 disease, especially in the elderly whose immune function is already more likely to be impaired. His paper, “Gut microbiome, Vitamin D, ACE2 interactions are critical factors in immune‑senescence and inflammaging: key for vaccine response and severity of COVID‑19 infection” describes the research showing how the status of the gut microbiome prior to COVID infection was highly predictive of inflammatory markers and the response to infection.
![]()
Reduced Risk of Death due to COVID-19 among Individuals with Higher Omega-3 Index
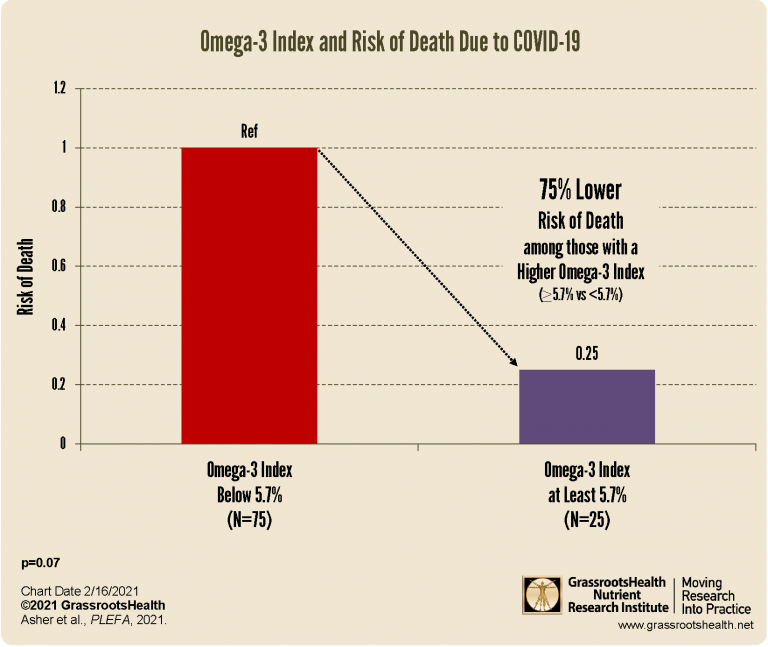
This small pilot study was published by Asher et al., and included 100 hospitalized COVID-19 patients whose blood was taken within ten days of diagnosis. When analyzing data between the highest quartile (with an Omega-3 Index of at least 5.7%, N=25) and the lowest quartiles (with an Omega-3 Index of below 5.7%, N=75), the authors found that the risk of death due to COVID-19 was approximately 75% lower in the group with the highest Omega-3 Index compared to those in the lower Omega-3 Index groups.
![]()
VIDEO: Vitamin D and Melatonin for COVID-19
In this video, Dr. Mobeen Syed interviews Dr. Paul Marik, MD, about vitamin D and melatonin, and how they may help with COVID-19. Dr. Marik is currently Professor of Medicine and Chief of Pulmonary and Critical Care Medicine at Eastern Virginia Medical School in Norfolk, Virginia, and is board certified in Internal Medicine, Critical Care Medicine, Neurocritical Care and Nutrition Science. Dr. Marik is the 2nd most published critical care physician in the world, having written over 500 peer-reviewed journal articles, 80 book chapters, and four critical care books; he has already co-authored 10 papers on therapeutic aspects of COVID-19. He has been cited over 43,000 times in peer-reviewed publications and has delivered over 350 lectures at international conferences and visiting professorships…
![]()
Selenium Status May Affect COVID-19 Outcomes
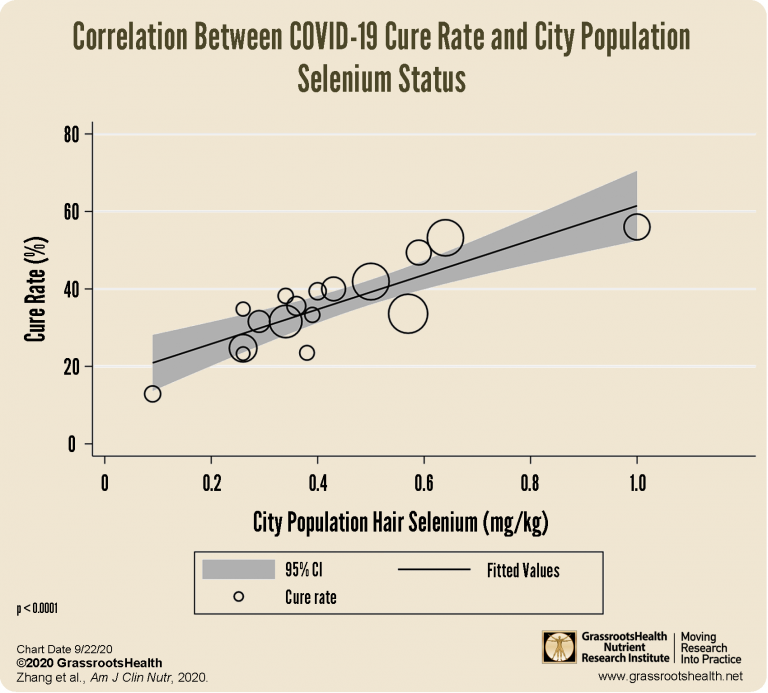
Several studies, such as those reviewed in a letter to the editor by Zhang et al., have related selenium deficiency to increased incidence of several different viral diseases and severity within certain populations. The authors found that the cure rate within Hubei province was statistically lower than all other provinces. They also found that one city within Hubei, a city well-known for its high selenium intake, had a higher cure rate than any other city within the province, at 36.4% (compared to an overall cure rate of 13.1% for the other cities combined, p<0.0001). When restricting the analysis to 17 cities outside of Hubei province, a significant association was found between the cure rate of COVID-19 and selenium status (p<0.0001).
![]()
Association between Dietary Patterns and Severity of COVID-19 Illness
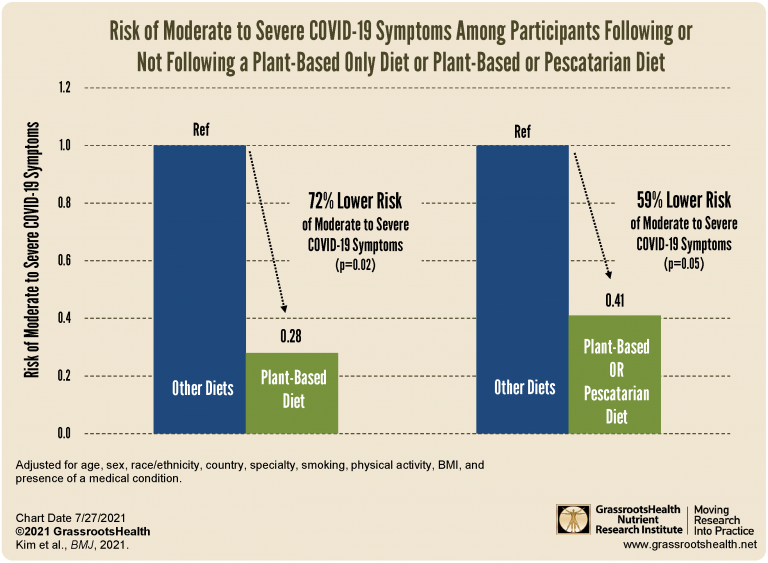
A study by Kim et al. evaluated the association between self-reported dietary patterns and COVID-19 infection, severity, and duration of symptoms among 2884 health care workers, all of whom had a high frequency of exposure to patients with COVID-19. Among the COVID-19 cases, 430 reported very mild to mild symptoms and 138 reported moderate-to-severe symptoms. Those who reported following a plant based diet had a 72% lower risk of moderate-to-severe COVID-19 illness compared to all other diets (p=0.02). Those in the plant based or pescatarian diet group had a 59% lower risk of moderate-to-severe COVID-19 illness (p=0.05).
![]()
Omega-3 Index Below 6.6% May be an Indicator of Immune System Imbalance
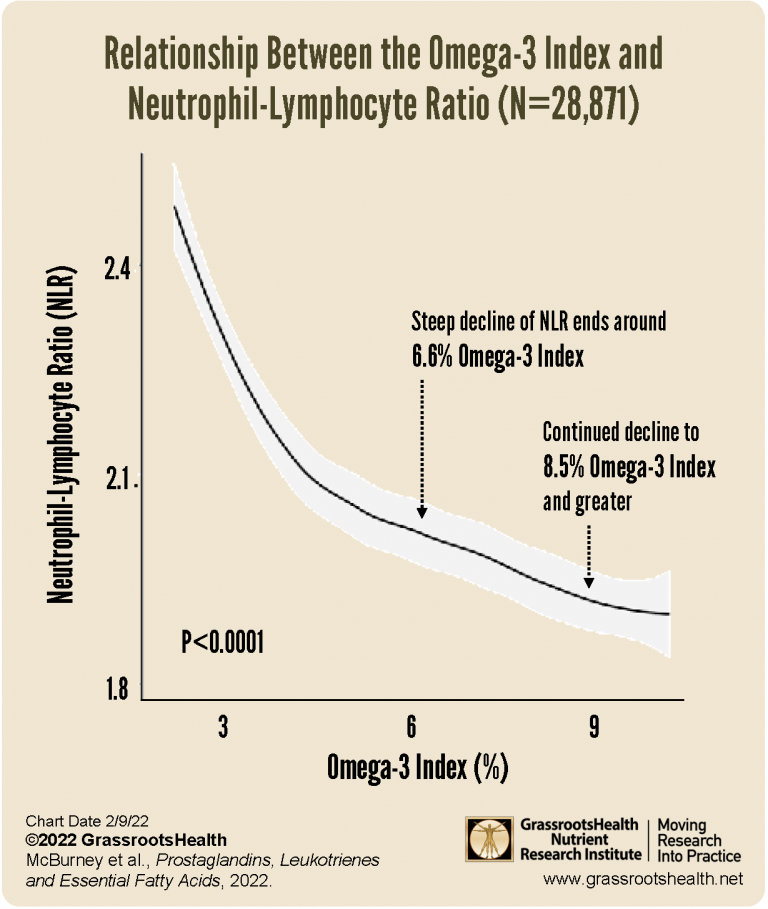
Omega-3s help mediate the immune response and are anti-inflammatory to help promote the resolution of the inflammatory process and prevent tissue damage due to inflammation. A recent study found an association between the Omega-3 Index and the NLR, indicating an Omega-3 Index > 6.6%, and possibly as high as 8.5%, is associated with lower NLR values that are indicative of a quiescent, balanced innate-adaptive immune system. The amount of neutrophils in comparison to the amount of lymphocytes is called the neutrophil-to-lymphocyte ratio (NLR), and it is an indicator of the balance between cells of the innate immune system and the adaptive immune system. A higher NLR (when neutrophil counts are high and lymphocytes are low) has been linked to increased systemic inflammation, and a 5.9% greater risk of severe COVID-19.
![]()
Vitamin D & Immune Function
How the Immune System Relies on Vitamin D
 How the Immune System Relies on Vitamin D
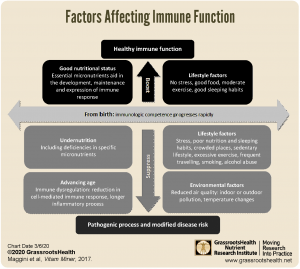
How the Immune System Relies on Vitamin DThe multiple important roles that vitamin D plays in immune function have been a major focus over the past year, especially in relation to COVID-19. As part of our What is Vitamin D Good For? series, this post will attempt to summarize those roles to clearly show how the immune system relies on vitamin D to function properly. Because vitamin D acts as a protector and regulator of all cell types, tissues, and organs, it is required for the proper functioning of each system of the body to help keep us healthy. This is especially true for our immune system, since vitamin D has specific regulatory effects on immune cells and inflammation.
![]()
Protective Role of Vitamin D against Coronavirus: Scientific Review and Dose for Immunity

This video by Dr. Renu Mahtani is clear, concise, and beautifully explains how vitamin D directly affects lung health, inflammation, and helps prevent viral attack.
![]()
Vitamin D, Immune System & SARS-CoV-2 (COVID-19)
 Vitamin D, Immune System & SARS-CoV-2 (COVID-19)
Vitamin D, Immune System & SARS-CoV-2 (COVID-19)This video by JJ Medicine discusses and clearly illustrates roles of vitamin D in immune system regulation, specifically with regards to how vitamin D can help protect against respiratory tract infections like SARS-CoV-2 (COVID-19). Included is a brief introduction to vitamin D and SARS-CoV-2, how vitamin D deficiency has been shown to increase the risk of all types of infections, how vitamin D supplementation has been shown to specifically protect against acute respiratory tract infections, and the ways vitamin D helps regulate the immune response during such infections.
![]()
How Vitamin D Helps Fight COVID-19: Part 1
 How Vitamin D Helps Fight COVID-19: Part 1
How Vitamin D Helps Fight COVID-19: Part 1This is a simplified review of how vitamin D helps to protect against COVID-19 infection and improve outcomes in those with COVID-19. Topics:
- Vitamin D is Known to Help Prevent Upper Respiratory Tract Infections
- Vitamin D Can Protect Lung Cells from SARS-CoV-2 Attack
- Vitamin D and ACE-2 Expression
- Vitamin D Regulates the Immune Response
![]()
Vitamin D Helps Fight COVID-19: Part 2
 Vitamin D Helps Fight COVID-19: Part 2
Vitamin D Helps Fight COVID-19: Part 2A continuation of the simplified review of how vitamin D helps to protect against SARS-CoV-2 infection and improve outcomes in those with active COVID-19. Topics:
- Effects of Vitamin D in Fighting a SARS-CoV2 Infection
- What Causes A Severe SARS-CoV-2 Infection?
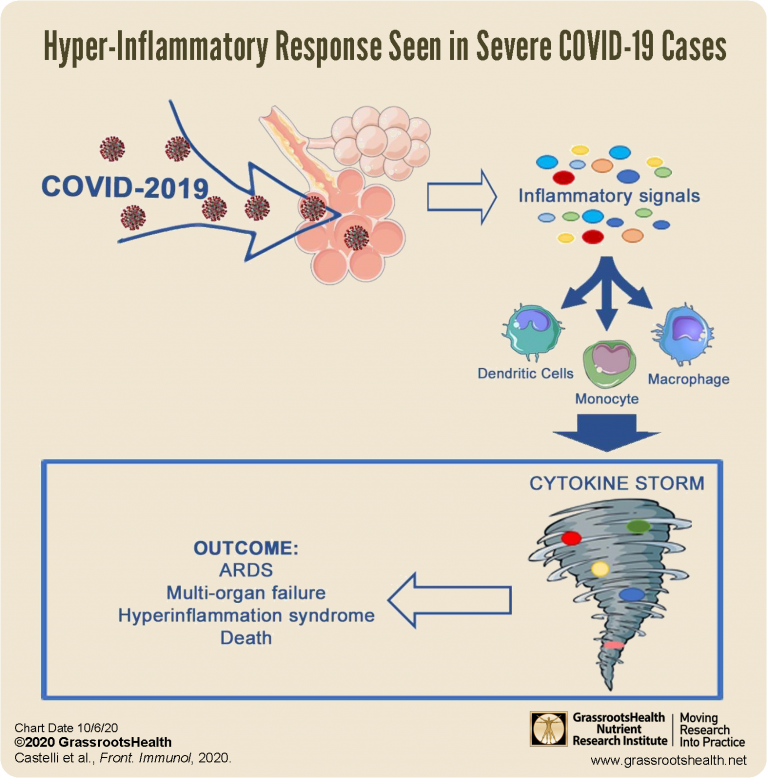
- Vitamin D Helps Control the Cytokine Storm and Reduce Symptom Severity
- More on How Vitamin D Regulates the Immune Response
![]()
Multisystem Inflammatory Syndrome (MIS-C) and Vitamin D in Children with COVID-19
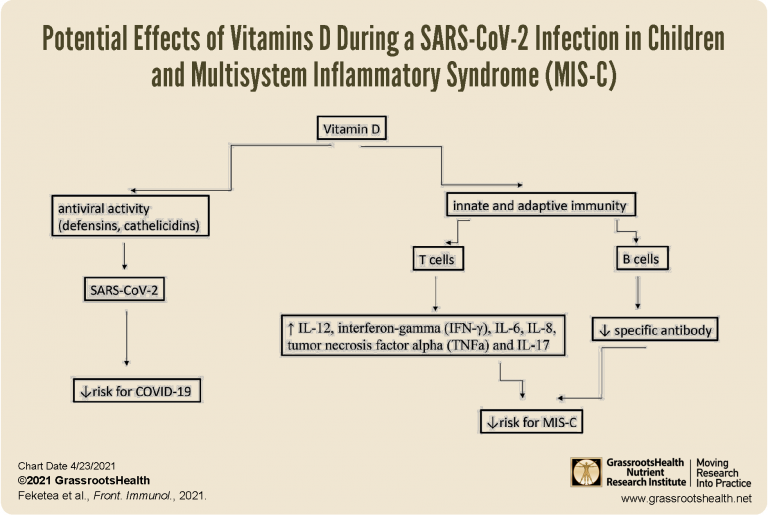
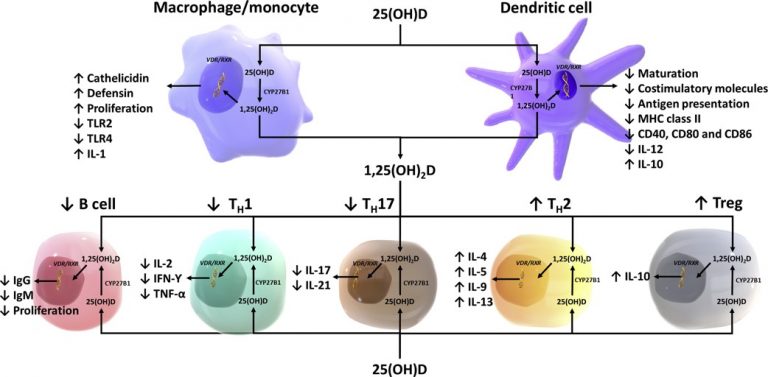
A review by Feketea et al. concludes that raising vitamin D levels could be effective in reducing the severity of MIS-C, as has been observed with another similar syndrome resulting from an excessive immune response to infection, Kawasaki disease. The authors illustrate just a few of the roles of vitamin D within the immune system during its response to a viral infection. The immune system relies on having a supply of vitamin D for specific needs, including increasing anti-inflammatory compounds and decreasing pro-inflammatory compounds – which is how it is able to reduce the severity of certain inflammatory reactions and decrease chances of cytokine storm.
![]()
Your Immune Cells Rely on Vitamin D
 Your Immune Cells Rely on Vitamin D
Your Immune Cells Rely on Vitamin DTopics:
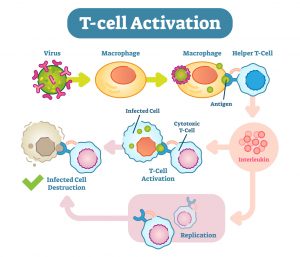
- Vitamin D Activates the T-cells for Immune Response
- How Does Your Immune System Work?
- The Innate vs Adaptive Immune Response
- The Role of T Cells in Destroying Viruses
- Is your immune system strong enough to help you stay healthy?
![]()
Vitamin D: An Orchestrator of Immune Responses
 Vitamin D: An Orchestrator of Immune Responses
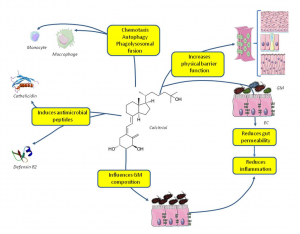
Vitamin D: An Orchestrator of Immune ResponsesActions of vitamin D:
- With immune and epithelial cells (such as those in the lungs and gastrointestinal tract)
- With white blood cells and pathogen destruction
- Immune modulating effects within the microbiota
![]()
Vitamin D and Immunity: Tying it All Together
 Vitamin D and Immunity: Tying it All Together
Vitamin D and Immunity: Tying it All TogetherMore Complex Vitamin D Dependent Functions in the Adaptive Immune Response
- Vitamin D is needed to activate T cells, turning naïve T cells into primed T cells that are better able to respond to a pathogen
- Vitamin D influences T cell differentiation to induce lower levels of inflammatory cytokines and higher levels of anti-inflammatory cytokines
- Vitamin D regulates the maturation of the dendritic cells, another type of white blood cells, to then modulate helper T cell (Th) function
- T cells respond directly to active vitamin D by developing regulatory T cells
![]()
Vitamin D3 Itself Creates Profound Anti-Inflammatory Effects
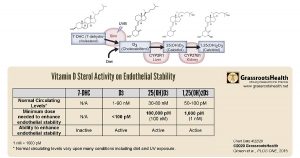
These authors discovered that vitamin D3 itself needed and taken in by the cells, and it is also actively used by the cells as a “potent and general mediator of endothelial stability at physiologically relevant levels.” Of particular note in the results was that vitamin D3, which was previously thought to be inactive, had the most potent effect – more than 10 times more potent than 1,25(OH)2D and more than 1,000 times more potent than 25(OH)D.
![]()
The ‘Other’ Pandemic
The Ignored Pandemic: Vitamin D Deficiency, by Dr. Eric Berg, DC, is a great, simple video to watch and share with others who may not have much education or background on vitamin D. The video quickly discusses:
- Overview of vitamin D’s importance
- Vitamin D’s various roles in the immune system
- Regulation of the inflammatory response (cytokine storm)
- How different immune cells rely on vitamin D
- Why are so many people deficient in vitamin D?? Reasons for deficiency
- Sun, skin color and vitamin D
![]()
Dr. Manson of Harvard Medical School and lead researcher: “Vitamin D may be more important now than ever”
“Vitamin D may be even more important now than ever,” says Dr. JoAnn Manson, MD, DrPH, of Harvard Medical School and Brigham and Women’s Hospital. Dr. Manson was the lead researcher and author of the VITAL trial and its resulting publications, which focused on the effects of supplemental vitamin D and omega-3s on specific health outcomes, mainly cancer and cardiovascular health. Now, with the current coronavirus epidemic, she is urging everyone to do what they can to avoid vitamin D deficiency, through sun exposure and supplements, due to emerging and growing evidence that vitamin D status may be related to the risk of developing COVID-19 disease and to its severity.
![]()
Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths
This paper is a review of the current research around the role of vitamin D in immune function, specifically in response to viral infections of the respiratory system. It outlines the relationship between vitamin D serum levels and the incidence of seasonal flu, as well as past epidemics such as those caused by the SARS and MERS coronaviruses. High risk conditions, the progression of illness, and mechanisms and proposed actions of vitamin D during the immune response are also reviewed.
![]()
Dr. Reinhold Vieth Presents Evidence of the Biology of Evolution to Demonstrate How a Person’s Skin Color Impacts Vitamin D Levels and Health Outcomes
For what reason could skin color have such a large effect on our health, to the extent that the mortality rate of COVID-19 is so much greater among dark skinned populations? In the video below, Dr. Reinhold Vieth clearly explains the history of the human species, our ability as a species to adapt and evolve to new environments, and how lighter skin is an example of such an adaptation in order to maintain our ability to survive and produce offspring.
![]()
Immune Function & Co-Nutrients
Nutrients to Support Vaccine Effectiveness
 Nutrients to Support Vaccine Effectiveness
Nutrients to Support Vaccine EffectivenessThere are many aspects of the immune response that require specific nutrients, regardless of whether that immune response is due to exposure to a pathogen or induced by a vaccination. When your body doesn’t get enough of these nutrients, the immune system is compromised and may not work at its full potential. This blog presents examples of how nutrients are involved in the immune response to a vaccine.
![]()
Immunity, Infection & Nutrients: What’s Missing from Public Discussions about COVID-19
 Immunity, Infection & Nutrients: What’s Missing from Public Discussions about COVID-19
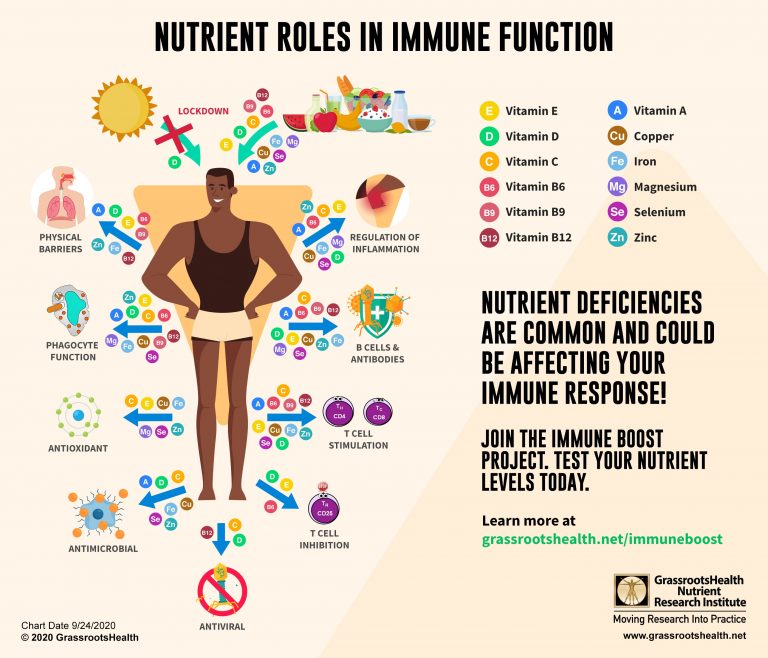
Immunity, Infection & Nutrients: What’s Missing from Public Discussions about COVID-19A new review by Uwe Grober and Michael Holick discusses several of these immune-relevant nutrients (Vitamin D, Vitamin A, Vitamin C, Selenium and Zinc) that “may help to increase the physiological resilience against COVID-19.” In other words, these nutrients play key roles in the body’s response to viral respiratory tract infections, including COVID-19, and may help protect against severe disease symptoms and outcomes.
![]()
Review Suggests Ensuring Adequate Zinc, Selenium and Vitamin D May Protect Against SARS-CoV-2
 Review Suggests Ensuring Adequate Zinc, Selenium and Vitamin D May Protect Against SARS-CoV-2
Review Suggests Ensuring Adequate Zinc, Selenium and Vitamin D May Protect Against SARS-CoV-2Certain nutrients, such as zinc, selenium, and vitamin D, are known to play a role in reducing inflammation and regulating the immune response. Deficiencies in these nutrients are known to impair immune function and also contribute to certain age-related diseases, such as diabetes, hypertension, and coronary heart disease, each of which are known risk factors for severe COVID-19. A review looked at current research and clinical data on the roles of zinc, selenium, and vitamin D within the immune system in response to viral infections of the lungs, and their potential impact on susceptibility to COVID-19. Included is a summary of the roles of each of these nutrients within our immune response, and how deficiency may hinder the effectiveness of that response.
![]()
Omega-3 Fatty Acids and COVID-19
 Omega-3 Fatty Acids and COVID-19
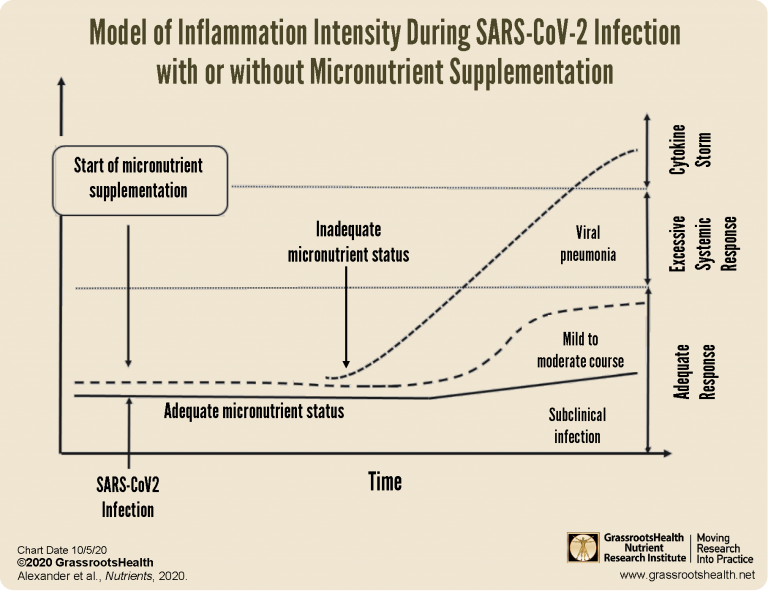
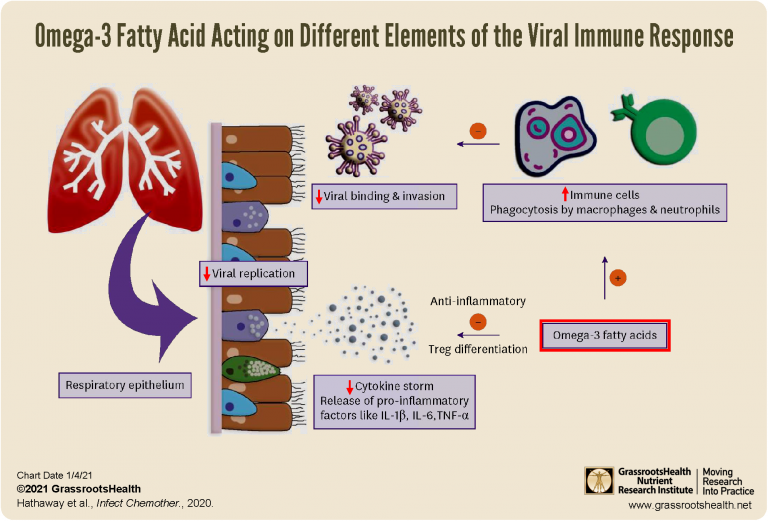
Omega-3 Fatty Acids and COVID-19This blog summarizes a review by Hathaway et al. that discusses the anti-inflammatory, immune-modulating, and potential antiviral roles of omega-3s and how they may contribute to the prevention of and response to COVID-19 disease. Omega-3 fatty acids may help prevent COVID-19 disease specifically by increasing the activity of immune cells needed to identify and destroy the virus, therefore decreasing the likelihood of viral binding and invasion; promoting T regulatory cell development and a controlled inflammatory process; and inhibiting inflammation, decreasing the production of inflammatory chemicals, and preventing a cytokine storm.
![]()
Direct Effects of Nutrient Deficiencies on Immune Function
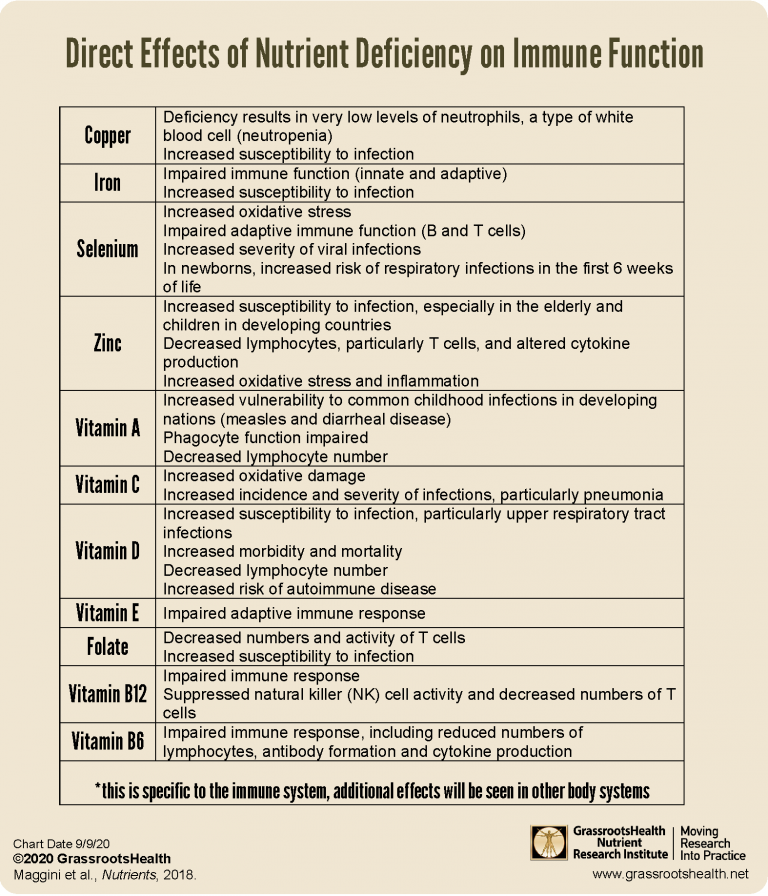 Direct Effects of Nutrient Deficiencies on Immune Function
Direct Effects of Nutrient Deficiencies on Immune FunctionIn this analogy, stilts are the pillars that your house of health is built upon, and many are required to keep the house stable and healthy. Being deficient in one or more nutrients weakens your stilts. Individual nutrient deficiencies have specific impacts on each stilt or body function and may impact other fibers in the stilt. The more deficiencies, the weaker each stilt becomes, allowing greater susceptibility to infection and disease – and the house falling. Providing your body with all the nutrients it needs is important for keeping your house of health supported. Learn more about individual effects of nutrient deficiencies on immune function.
![]()
Nutrient Deficiencies are a Major Health Concern!
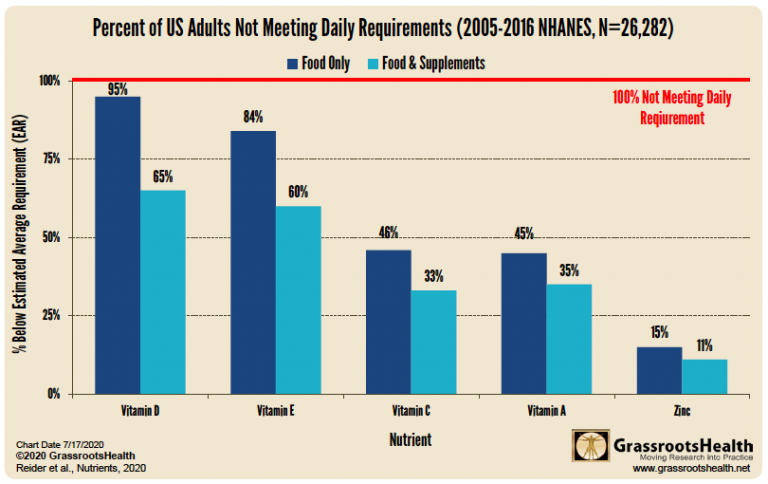 Nutrient Deficiencies are a Major Health Concern!
Nutrient Deficiencies are a Major Health Concern!A recent review by Reider et al. analyzed the latest set of NHANES data to get a better idea of nutrient intake. Specifically, they looked at Vitamins A, C, D, E and zinc due to their well-known roles in immune function. The results show what the inadequate intakes are for each nutrient, based on intake from food alone and from food plus dietary supplements. While supplements do help bridge the gap for some, many are still left with inadequate intake of several key nutrients.
![]()
Nutrients Have an Integral Role in Immune Function
 Nutrients Have an Integral Role in Immune Function
Nutrients Have an Integral Role in Immune FunctionOne of the primary reasons for the current issue with the Coronavirus (SARS-CoV-2) pandemic is that so many people do not have a healthy enough immune response to protect them when they get exposed to the virus. Your nutritional status plays a central role in how your body functions and responds to daily lifestyle and environmental factors. Vitamins and minerals play integral roles in all body functions and are integral to your health. We want everyone to be ‘exposed’ to this information and to know that they can take action to help themselves be healthy—NOW!
![]()
Omega-3 Fats from Fish Oils May Help LOSS OF SMELL
This video is another by Dr. Susan Brown of Better Bones, introducing a very interesting topic – that omega-3 fats from fish oils can have a profound effect on the loss of smell, new research shows.
![]()
How Your Immune System Protects You From Infections
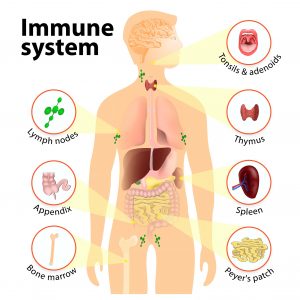 How Your Immune System Protects You From Infections
How Your Immune System Protects You From InfectionsYour immune system has been training since you were born to protect you from the “pathogens” that cause infection or disease. But sometimes, infection takes hold and your immune system has to fight off those pathogens. What you may not realize is that the nutrients in your diet directly influence the ability of your immune system to function. This is a review of the first and second lines of defense used by the immune system, immune memory, and the role different nutrients play within specific immune functions.
![]()
How Your Immune System Protects You From Infection – Part 2: Phagocytes
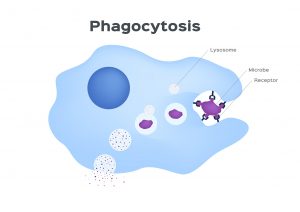 How Your Immune System Protects You From Infection – Part 2: Phagocytes
How Your Immune System Protects You From Infection – Part 2: PhagocytesThere are chemical factors (complement, acute-phase proteins and cytokines) and several types of non-specific immune cell types that roam around in the blood and tissues of the body on the look-out for pathogens (bacteria and viruses that cause disease). These non-specific immune cells, called “phagocytes,” are a key component of the first line of defense and the focus of this article. Phagocytes, through a process called phagocytosis, gobble up (engulf) and kill (digest) bad bugs (pathogens) when they recognize them. The process requires a balance of specific nutrients in order to function, and may be hindered when those nutrients are deficient.
![]()
How Your Immune System Protects You From Infection: Part 3 – B cells & Antibodies
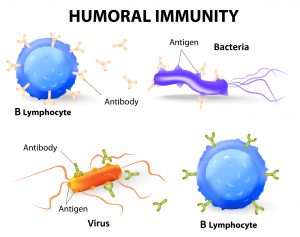 How Your Immune System Protects You From Infection: Part 3 – B cells & Antibodies
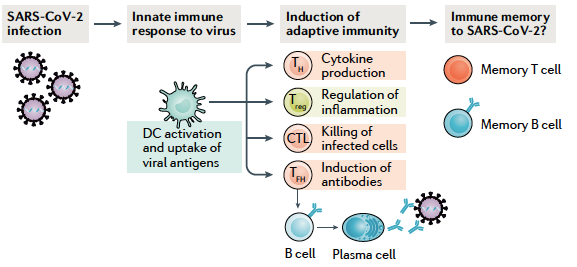
How Your Immune System Protects You From Infection: Part 3 – B cells & AntibodiesThe development of immunity to a pathogen through natural infection is a complex process that typically takes place over a couple of weeks and involves the innate and adaptive immune systems. The body responds immediately with a non-specific innate response in which phagocytes work to slow the progress of the infection and may prevent it from causing symptoms. This non-specific innate response is followed by an adaptive response. Today’s post will focus on humoral immunity (or the part of the immune response involving memory of a previous pathogen) and the production of antibodies.
![]()
How Your Immune System Protects You From Infection: Part 4 – T lymphocytes
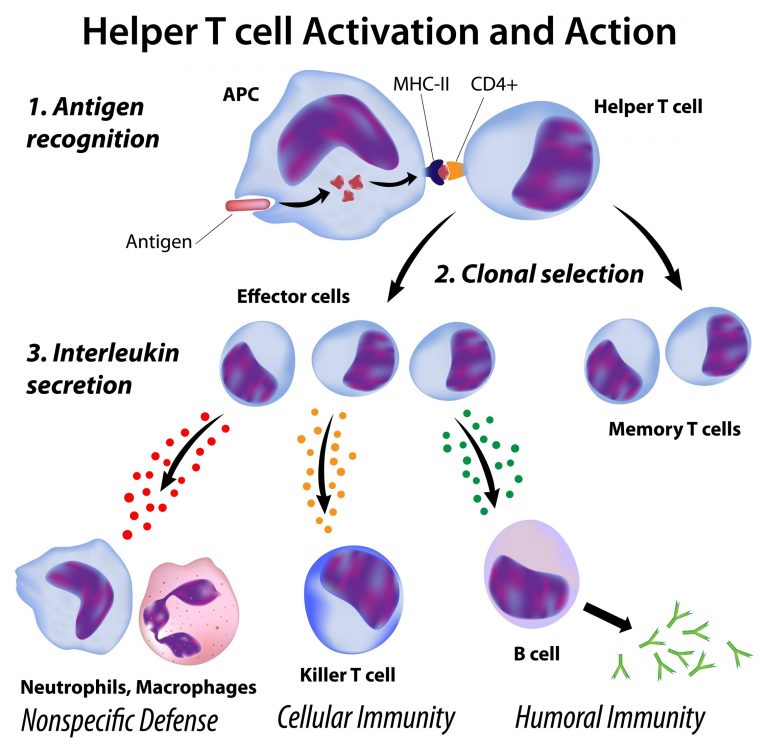 How Your Immune System Protects You From Infection: Part 4 – T lymphocytes
How Your Immune System Protects You From Infection: Part 4 – T lymphocytesThe adaptive immune system starts to work after the innate immune system is activated. If an infection progresses despite the inflammation, fever, and phagocyte activity of the innate immune system, a more coordinated response is required in order to destroy the pathogen. T cells orchestrate cells from both the innate and adaptive immune systems in an attempt to overcome the pathogen.
![]()
A Healthy Immune Response Relies on Your Nutrient Status
 A Healthy Immune Response Relies on Your Nutrient Status
A Healthy Immune Response Relies on Your Nutrient Status“There is a close relationship between nutritional status and immune function. Hence, immunocompetence can be regarded as a measure of adequate nutrition.” This post reviews how the immune system relies on the following nutrients:
- Vitamin C
- Vitamin D
- Zinc
![]()
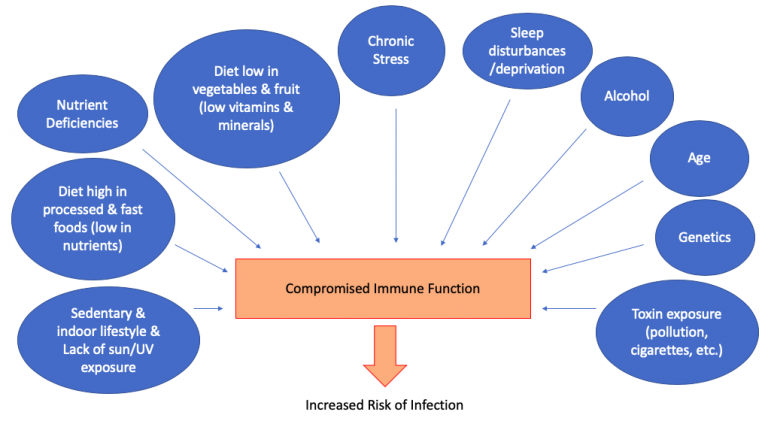
Immune Response Affected by Nutrient Status and Other Factors
 Immune Response Affected by Nutrient Status and Other Factors
Immune Response Affected by Nutrient Status and Other FactorsThe following are additional factors to consider for maintaining healthy immune function:
- Age
- Environmental Temperature
- Air Pollution
- What’s the Bottom Line?
- What’s the Main Action to Take?
![]()
Low Hemoglobin and Vitamin D Deficiency Could Contribute to Severity of Respiratory Infections
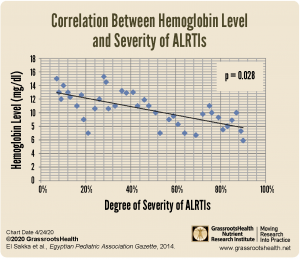
Iron deficiency anemia is another risk factor that may increase the severity of respiratory tract infection, especially in those that are vitamin D deficient, as found in a study by El Sakka et al. of 96 hospitalized infants and 96 healthy controls. Iron deficiency anemia is the most common micronutrient deficiency worldwide and acute lower respiratory tract infection (ALRTI) is a major cause of illness and death in developing nations where incidence of anemia is high.
![]()
Improving Zinc Levels to Improve Immune Function

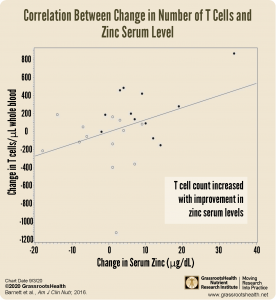
A randomized, double-blind, placebo controlled study identified 31 elderly individuals (ages 65 and older) in nursing homes with low zinc levels who were assigned to receive either 30 mg of zinc per day (n=15) or a placebo with only 5 mg zinc per day (n=16). Those in the zinc group experienced improvements in lymphocyte proliferation and saw a significant increase in the number of T cells. A correlation was found between the change in zinc concentration, lymphocyte proliferation (p=0.02), and the number of T cells in the blood (p=0.06). Combined with the importance of T cells for resisting infection, this study suggests that improving zinc status in those who are deficient may help to reduce the risk of infections such as pneumonia.
![]()
Flu, Colds & Other Respiratory Infections
Up to 70% Lower Risk of Acute Respiratory Tract Infections with Vitamin D Supplementation
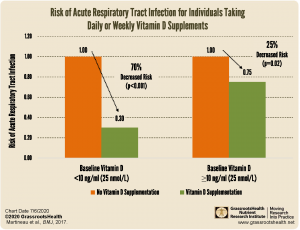
In a meta-analysis published in 2017, Martineau et al. set out to assess the effect of vitamin D supplementation on the risk of acute respiratory tract infection (RTIs). The review included 25 randomized, double-blinded, placebo controlled trials (RCTs), with a total of 11,321 individual participants. They found that vitamin D supplementation resulted in a statistically significant reduction in risk of RTIs among all participants, with a 12% lower risk of acute RTIs for those supplementing with vitamin D versus those with no supplementation. The greatest protective effect was seen among participants who received daily or weekly supplementation and whose starting vitamin D level was less than 10 ng/ml (25 nmol/L), with a 70% decreased risk of acute RTI with vitamin D supplementation compared to a 25% reduction for those whose starting levels were greater than 10 ng/ml.
![]()
Acute Respiratory Distress Syndrome (ARDS) Directly Influenced by Vitamin D
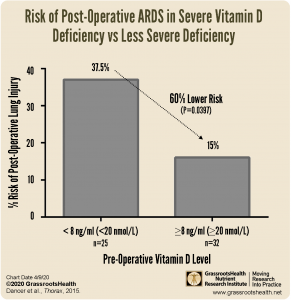
Acute Respiratory Distress Syndrome (ARDS, aka wet lung) is a condition resulting from severe respiratory injury or illness, such as pneumonia, in which the air sacs of the lungs fill with fluid, preventing the uptake of oxygen. The condition leads to shortness of breath and difficulty breathing, and in severe cases, can lead to sepsis and/or death. ARDS is currently a major complication and cause of death among those with serious COVID-19 infections. When comparing vitamin D levels among those with and at risk of ARDS, it was found that 96% of those at risk of ARDS were deficient in vitamin D, and surgery patients with severe vitamin D deficiency had a 37.5% risk of lung injury post-surgery compared to a 15% risk for those whose vitamin D level was above 8 ng/ml (20 nmol/L), a 60% lower risk for those with higher vitamin D levels.
![]()
Fewer Respiratory Tract Infections in Infants with Daily Supplementation of Vitamin D
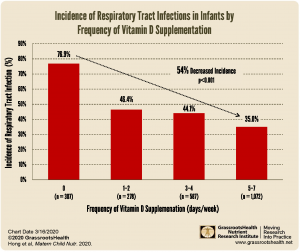
- infants who received supplementation 5-7 days per week were 54% less likely to get an RTI than those who did not receive any supplementation with vitamin D; risk of RTIs went down as the frequency of vitamin D supplementation increased.
- Risk of any RTI, lower RTI, or RTI related hospitalization was reduced for infants receiving vitamin D supplementation, regardless of whether they were breastfed or formula fed.
- Among infants who were diagnosed with an RTI, those who received any vitamin D supplementation developed their first RTI later than those who did not receive any vitamin D supplementation.
- Infants receiving vitamin D supplementation at least 5 days per week had the best outcomes.
![]()
Could More Solar UVB Exposure Decrease Flu Fatalities?
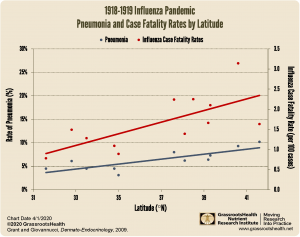
A general trend can be seen with lower rates of pneumonia as a complication of influenza and influenza fatalities for those locations at lower latitudes within the United States where vitamin D production from UVB is more. This is consistent with a number of other papers published showing a decrease in other conditions closer to the equator–from type 1 diabetes to breast cancer.
![]()
Cold and Flu Season is Approaching (Part 4)
 Cold and Flu Season is Approaching (Part 4)
Cold and Flu Season is Approaching (Part 4)What else, besides vitamin D, might help decrease the risk of getting a cold or flu, or the time and severity of symptoms if you do get sick?
- Could Omega-3s Make a Difference for Colds and Flu?
- What about Zinc?
- Is the flu vaccine the best way to protect against the flu?
![]()
Could Your Immune System Benefit from Vitamin D?
Make sure you know your vitamin D level, and take steps to keep it within a target of 40-60 ng/ml or 100-150 nmol/L! Through GrassrootsHealth Nutrient Research Institute, you can also test your essential elements magnesium, copper, zinc and selenium, toxins such as lead, mercury and cadmium, as well as your omega-3 levels, inflammation levels and thyroid stimulating hormone (TSH) level. Find out your levels today! Log on to the test selection page (click the link below) to get your tests and see for yourself if your levels can be improved.
Make sure you track your results before and after, about every 6 months!
Click Here to Access the Test Page
How can I track my nutrient intake and levels over time?
To help you track your supplement use and nutrient levels, GrassrootsHealth has created the Personal Health Nutrient Decision System called

For each specific supplement, you can track what days you take it, how much, and many other details. This will help you know your true supplemental intake and what patterns of use work for you to reach and maintain optimum nutrient levels. Check it out today!