Dear Reader,
An update to Vitamin D Guidelines recently issued by the Endocrine Society (June 2024), titled “Vitamin D for the Prevention of Disease: An Endocrine Society Clinical Practice Guideline,” is a step backward and requires urgent and necessary action from all researchers, educators, healthcare workers, and advocates in the vitamin D scientific community.
For a short explanation of these updated guidelines, read their list of recommendations included here, the Endocrine News article here, or watch the Endocrine Society’s press conference video here.
These updated guidelines suggest that most adults should take no more than the recommended daily allowance as set by the outdated (2011) Institute of Medicine (IOM) document. This recommendation has led to massively high rates of deficiency and associated diseases, harming the population. In addition, the new guidelines do not support testing 25(OH)D levels among any population, even for the vulnerable, nor do they define a sufficiency level. This recommendation is short-sighted, dangerous, and confusing. It is a significant step backward from what the Endocrine Society previously recommended for vitamin D in 2011.
It is time to collaborate to counter these erroneous public health recommendations before additional harm is done to the health of individuals.
Over fifteen years ago, GrassrootsHealth founder Carole Baggerly took action to define a scientific consensus, through the agreement of 40 leading vitamin D scientists and researchers, that the vitamin D level necessary for the optimal human health of the general population should be 40-60 ng/ml (100-150 nmol/L). Back then, it was well known among vitamin D experts that the recommendations made by the IOM were inadequate to support these levels and were part of the driving force behind the worldwide vitamin D deficiency epidemic. She met with vitamin D researchers and scientists across the US and Canada to create the first Scientists’ Call to D*action to solve the vitamin D deficiency epidemic and improve public health. This was primarily via promoting vitamin D inputs necessary to achieve and maintain a target 25(OH) vitamin D serum level of 40-60 ng/ml (100-150 nmol/L). Since then, 48 senior vitamin D researchers have signed this Call to Action.
We have since gained more than 15 years of additional research and findings from peer-reviewed publications to support and validate this recommended target vitamin D level of 40-60 ng/ml, the vitamin D doses necessary to achieve it safely and effectively, and the newly updated (2024) Scientists’ Call to D*action.
Scientists’ Call to D*action – The Vitamin D Deficiency Epidemic
40-75% of the world’s population is vitamin D deficient at any given time
[The Scientists’ Call to D*action was first issued in 2008 and last updated in 2024]
The causal link between severe vitamin D deficiency and rickets or the bone diseases osteomalacia, osteopenia, osteoporosis, and increased risks for falls and fractures is overwhelming.
Research has highlighted the newly appreciated, vital associations between vitamin D insufficiency or deficiency and extra-skeletal diseases. Examples of these include breast cancer, intestinal and other cancers, multiple sclerosis, Type 1 diabetes, metabolic disorders such as Type 2 diabetes and metabolic syndrome, hypertension, increased risk of heart failure, prenatal and neonatal complications, and acute infections, including having a beneficial impact on survival and hospitalization in influenza and SARS-CoV-2, and a favorable role in treating chronic infections such as tuberculosis and moderation of inflammatory bowel disease. Recommended daily intakes as set by the Institute of Medicine (IOM) in 2011 are too low to adequately support the role of vitamin D for such extra-skeletal processes and disorders mentioned above, leading to increased risk of such diseases, even in healthy people.
Based on the evidence we now have at hand, action is warranted.
It is projected that the incidence of many of these diseases could be reduced by 20%-50% if vitamin D deficiency is eradicated by increasing vitamin D3 intakes through fortified foods or vitamin D3 supplements, or with daily moderate safe sun exposure when feasible based on skin type, medical history, and latitude.
The established way to determine vitamin D status is by measuring the serum 25-hydroxyvitamin D [25(OH)D] concentration. Testing is indicated among specific groups of individuals based on bodyweight, disease status, digestive health, life stage, concurrent medications, and other factors. The intake of vitamin D3 required for sufficiency and resulting substantial disease reduction and to prevent complications of disease depends on the individual’s age, race, lifestyle, latitude of residence, genome, bodyweight, BMI, and other factors. The latest IOM report from 2011 indicates 10,000 IU/day is considered the NOAEL (no observed adverse effect level). While 4000 IU was regarded as the safe upper intake level for 9 years and older, research has shown no toxicity from vitamin D below a serum 25(OH)D level of 125 ng/ml (312 nmol/L).
It is well-documented that the darker the skin, the less vitamin D is produced in the skin, and thus, the higher the risk of vitamin D deficiency. Even in southern US climates, at least 55% of African Americans and 22% of Caucasians are vitamin D deficient, and they are vulnerable to developing new disorders and worsening existing diseases.
More than 4.5 billion people worldwide are affected at some time of the year by vitamin D deficiency, resulting in many adverse health events and premature deaths.
This Scientists’ Call to D*action is issued to alert the public and medical community to the importance of maintaining serum vitamin D levels—25(OH)D—between 40 and 60 nano-grams/milliliter (100-150 nanomoles/liter) to reduce risks of and help prevent these diseases and their complications. Recommended doses of vitamin D are those necessary to achieve and maintain this target serum level of 25-hydroxyvitamin D. Implementing this would be safe, effective, and inexpensive.
Adequate vitamin D status will promote better health, leading to a healthier population, less sickness, a more productive workforce, and substantially reducing health care costs.
The D*action project aims to serve as a model for public health action on vitamin D and is a scientific test bed for techniques and outcome evaluations at a community level.
Donate to Support this Effort Here
Stay tuned for more on how you can help support this effort and help combat the confusing and harmful information contained in these updated guidelines.
Endorsements of the GrassrootsHealth Call to D*action (Our Original Scientists’ Panel and Updated Endorsements 2024)
Published Vitamin D Scientists
John Adams, MD (United States)
Professor, Department of Medicine, Molecular, Cell, and Developmental Biology
Orthopedic Surgery, University of California Los Angeles
Cedric Annweiler, MD, PhD (France)
Associate Professor of Geriatric Medicine and Biology of Aging, University of Angers, France
Linda Benskin, PhD, RN, SRN (Ghana), CWCN, CWS, DAPWCA, WOCNF (United States)
Benskin Research Group and Ferris Mfg. Corp.
Carlos A. Camargo, Jr, MD, DrPH (United States)
Professor in the Department of Epidemiology, Harvard Medical School
John J. Cannell, MD (United States)
Executive Director, Vitamin D Council
Heide S. Cross, PhD (Austria) †
Vienna Medical University – retired
Ana Maria Fernandez Alonso, MD (Spain)
Torrecardenas Hospital, Almeria
Milan Fiala, MD (United States)
Research Professor, Orthopedic Hospital Research Center, University of California Los Angeles
Leigh Frame, PhD, MHS (United States)
George Washington University
Richard L. Gallo, MD, PhD (United States)
Professor of Medicine and Pediatrics, and Chief of the Division of Dermatology, University of California San Diego
David Gardner, MS, MD (United States)
Professor, University of California San Francisco School of Medicine
Cedric Garland, DrPH, FACE (United States)
Professor, University of California San Diego Department of Preventive Medicine
Principal Investigator, GrassrootsHealth
Frank C. Garland, Ph.D. † (United States)
University of California, San Diego
Edward Giovannucci, MD, ScD (United States)
Harvard School of Public Health Professor of Nutrition and Epidemiology
Adrian F. Gombart, PhD (United States)
Principal Investigator, Linus Pauling Institute, Oregon State University, Associate Professor, Department of Biochemistry and Biophysics
Edward Gorham, PhD (United States)
Associate Professor in the Department of Family Medicine and Public Health, University of California San Diego
William B. Grant, PhD (United States)
Director, Sunlight, Nutrition, and Health Research Center
Bernard P. Halloran, PhD (United States)
Senior Career Scientist, Veterans Affairs Medical Center and Adjunct Professor, Department of Medicine, University of California San Francisco
Bruce D. Hammock, PhD (United States)
Distinguished Professor of Entomology, University of California Davis
Tissa Hata, MD (United States)
Clinical Professor in the Division of Dermatology, University of California San Diego
Robert P. Heaney, MD † (United States)
Professor of Medicine, Creighton University
Former Research Director, GrassrootsHealth
Martin Hewison, PhD (United Kingdom)
Professor of Molecular Endocrinology, University of Birmingham
Michael F. Holick, MD, PhD (United States)
Professor of Medicine, Physiology and Biophysics Boston University School of Medicine
Bruce W. Hollis, PhD (United States)
Professor of Pediatrics, College of Medicine, Medical University of South Carolina
Benjamin Jacobs, MD (United Kingdom)
Royal National Orthopaedic Hospital, Consultant Paediatrician
Candace Johnson, PhD (United States)
President & CEO Wallace Family Chair in Translational Research, Professor of Oncology, Roswell Park Cancer Institute
Spyridon Karras, MD, PhD (Greece)
Endocrinologist, Research Coordinator, Ahepa University Hospital, Thessaloniki, Greece
Samantha Kimball, PhD (Canada)
Research Director, GrassrootsHealth
H. Phillip Koeffler, MD (United States)
Professor, Department of Medicine, Hematology Oncology, University of California Los Angeles
Kalliopi Kotsa, MD, PhD (Greece)
Assistant Professor of Endocrinology, Ahepa University Hospital, Thessaloniki ,Greece
Joan M. Lappe, PhD, RN, FAAN (United States)
Director of Clinical and Pediatric Studies, Professor, Department of Medicine, Division of Endocrinology, Creighton University
Bonnie Mallard, PhD (Canada)
Professor of Immunology and Immunogenetics, University of Guelph
José Luis Mansur, MD (Argentina)
Médico especialista en Endocrinología y Osteología
Past President de la Sociedad Argentina de Osteoporosis
Director del Centro de Endocrinología y Osteoporosis La Plata, Argentina
Patrick McCullough, MD (United States)
Chief of Medical Services, Summit Behavioral Health
Tetsuya Mizoue, MD, PhD (Japan)
National Center for Global Health and Medicine, Director, International Medical Center of Japan
Mathew T. Mizwicki, PhD EMBA (United States)
Baxter International
Anthony W. Norman, PhD † (United States)
Distinguished Professor of Biochemistry & Biomedical Sciences, Emeritus, University of California Riverside
Keith C. Norris, MD, PhD (United States)
Professor of Medicine, University of California Los Angeles Division of General Internal Medicine and Health Services Research
Beatriz Oliveri, MD, PhD (Argentina)
Researcher CONICET (National Council of Scientific and Technical Research Council -Argentina)
Head Laboratory of Osteoporosis and Bone Metabolic Diseases-Hospital de Clinicas-University of Buenos Aires- Argentina
Ex Presidente Asociación Argentina Osteología y Metabolismo Mineral (AAOMM)-(período 2007-2009)
Médica Staff- Mautalen-Salud e Investigación
Faustino R. Pérez-López, MD, PhD (Spain)
Aragon Health Research Institute, University of Zaragoza Faculty of Medicine, Zaragoza
Stefan Pilz, MD (Austria)
Medical University of Graz
Pawel Pludowski (Poland)
Professor, The Children’s Memorial Health Institute, Warsaw, Poland
A. Hari Reddi, PhD (United States)
Professor Ellison Chair of Orthopaedic Research Orthopedics, Medical Center/School of Medicine, University of California Davis
Ray Rodriguez, PhD (United States)
Professor, Department of Molecular & Cellular Biology, University of California Davis
Laura P. Schoepf, PhD (United States)
Assoc. Faculty at Mt. San Jacinto College
Gerry Schwalfenberg, MD, CCFP (Canada)
University of Alberta
Robert Scragg, MD, PhD (New Zealand)
Head of Department, Epidemiology & Biostatistics, University of Auckland
Joerg Spitz, MD (Germany)
Society for Medical Information und Prevention
Vin Tangpricha, MD, PhD (United States)
Distinguished Physician, Professor of Medicine, Emory University School of Medicine
Donald L. Trump, MD, FACP (United States)
CEO & Executive Director, Inova Dwight and Martha Cancer Institute, Comprehensive Cancer and Research Institute
Reinhold Vieth, PhD (Canada)
Departments of Laboratory Medicine, Pathobiology and Nutritional Sciences
University of Toronto, Mt Sinai Hospital
Raimund von Helden, MD (Germany)
Institute VitaminDelta
Carol Wagner, MD (United States)
Professor of Medicine, Neonatologist, Associate Director, Neonatal-Perinatal Fellowship Program and Translational Research Center Medical University of South Carolina
JoEllen Welsh, PhD (United States)
Empire Innovations Professor, Cancer Research Center, University at Albany – SUNY
John H. White, PhD (United States)
Professor, Departments of Physiology and Medicine, McGill University
Susan J. Whiting, PhD (Canada)
Professor of Nutrition and Dietetics, University of Saskatchewan
Walter C. Willett, DrPH, MD
Fredrick John Stare Professor of Epidemiology and Nutrition, Chair, Department of Nutrition, Harvard School of Public Health
Sunil Wimalawansa, MD, PhD, MBA (Sri Lanka)
Professor of Medicine, Endocrinology & Nutrition
Alexander Wunsch, MD (Germany)
Wismar University of Applied Sciences
Health Professionals and Practitioners
Janice Blanke, DC (Canada)
Perry Holman (Canada)
Executive Director, Vitamin D Society
Mha Atma S Khalsa, DC (United States)
Marie-Helene Lessard (Canada)
Naturopath, IESN
Katherine Locke, RN, BSN, post-bacc cert.; MSN (United States)
Victoria Meakin, MB, ChB, MRCGP (Great Britain)
Julianne North, MD, MPH (United States)
University of San Diego
Thomas Reynolds, MD, FACS (United States)
American Academy of Ophthalmology
Troy Ross, MD, MPH (United States)
Public Health Officer
Charli Van Horn, RN, BS (United States)
Wolfgang Walter, MD, MRCGP (Great Britain)
National Health Service
Additional Endorsements
Jennifer Aliano, MS (United States)
Director, GrassrootsHealth
Daniel Arnaud (United States)
Carole Baggerly (United States)
Founder, GrassrootsHealth
Tero Brandstaka (Finland)
Kalle Pihlajasaari, BSc (Finland)
https://cholecalciferol.miraheze.org/wiki/Kalle_Pihlajasaari
Comments from Published Vitamin D Scientists & Researchers
As an immunologist it seems clear to me that to optimize immune function it is critically important to test vitamin D levels and then adjust supplementation accordingly. Test, don’t guess.
Bonnie Mallard, PhD (Canada)
It’s a simple dose response problem. The Endocrine Society is stuck on the flat, no response part of the dose response curve, because the studies that they review use inadequate amounts of vitamin D. They exclude analysis of studies that show a clinical benefit from vitamin D, sunshine, and UVB phototherapy, and the corresponding serum 25OHD concentrations.
In the 1930s and 1940s, when vitamin D was first shown to be an effective treatment for asthma, psoriasis, RA, and TB, investigators were using supraphysiologic doses of vitamin D, ranging from 60,000 to 600,000 units a day, and were on the opposite, effective flat part of the dose response curve, where side effects become a risk. Hypercalcemia was a common problem in the 1930s and 1940s because the vitamin D doses used were much more than were necessary to treat these diseases.
There are very many well documented health benefits from vitamin D if you use enough or get adequate exposure to sunshine or UVB radiation. Sunshine and UVB radiation work in treating psoriasis and TB by restoring adequate vitamin D status. With adequate vitamin D status, the genes can be activated that make antimicrobial peptides that cure TB infections, and other genes that make and maintain the functional status of regulatory T lymphocytes, which control autoimmune diseases.
The best estimates for vitamin D production in the skin from adequate daily sun exposure range from 10,000 to 25,000 units a day. These were made in the 1970s and 1980s. In 2010 a study showed that vitamin D regulates about 3000 protein coding genes.
When I discovered this data in 2009 and 2010, I sought to replicate the results reported in the 1930s and 1940s using vitamin D intake ranging from 10,000 to 40,000 units a day. It proved to be very safe effective in my experience, in treating asthma, psoriasis, Crohn’s disease, MS, RA, ulcerative colitis, Graves’ disease, urticaria, and Lichen planus in friends, colleagues, and patients.
The sweet spot for maximal vitamin D efficacy with no hypercalcemia appears to be between 10,000 to 50,000 units a day. This would be the rising part and beginning of the plateau of the dose response curve.
In 2019 one of Dr. Michael Holick’s many fantastic reports showed that after 6 months of daily intake, gene regulation varied significantly between 600, 4000, and 10,000 units in 3 groups of healthy volunteers. The number of genes up or downregulated in the 3 groups were 162, 320, and 1289. This explains why the dose response curve is flat with lower daily intakes of vitamin D. It’s not enough vitamin D to meet the needs of the body. I asked Michael if he could repeat the 2019 study using 20,000 and 30,000 units of vitamin D a day, to see where the number of genes up or down regulated by vitamin D plateaus. That would be very interesting data to see. I continue to take 55,000 units a day with no complications.
Hypercalcemia from excessive vitamin D intake does not appear to occur until the serum 25OHD gets above 400 ng/ml, and my clinical experience is consistent with this. The highest serum 25OHD concentration observed post UVB treatment of a psoriasis patient that I could find was 159 ng/ml, reported in 1996. I mention this because it speaks to the safety of vitamin D.
Dr Patrick McCullough, MD (United States)
Since some years ago, the association between 25OHD deficiency and various non-skeletal diseases is clear. Healthy people with a deficiency are more likely to develop diseases over time. Why be satisfied with having a 25OHD level that ensures bone health when a higher dose could prevent other pathologies without risk? And they claim there were no large studies of supplementation against placebo (RCT) that demonstrated prevention or relief of nonclassical pathologies or diseases?
Now there are two large studies in which supplementation was carried out in the general population (VITAL and D2d). They showed, in the reanalysis, prevention of cancer mortality and the apparent onset of autoimmune disease in the first, and prevention of the transition from prediabetes to diabetes in subjects who reached a level of 40 ng/ml of 25OHD in the second. Other studies also showed positive responses of vitamin D supplementation or positive effect of levels equal to or greater than 40 ng/mL (inflammatory bowel diseases, multiple sclerosis, etc). But it seems that these very important data are ignored by the scientific community. Why? Are there economic reasons as the only justification for recommending not measuring 25OHD in risk groups such as pregnancy? Our opinion is in this article: Mansur JL, Oliveri B, Giacoia E, Fusaro D, Costanzo PR. Vitamin D: Before, during and after Pregnancy: Effect on Neonates and Children. Nutrients. 2022 May 1;14(9):1900.
Dra Beatriz Oliveri & Dr José Luis Mansur (Argentina)
Just because we don’t have the science nailed down, doesn’t mean we shouldn’t improve vitamin D status in those we know are at risk. These new guidelines are short-cited.
Leigh A. Frame, PhD, MHS (United States)
Comments from Medical Doctors and Health Care Practitioners
My clinical experience with patients and vitamin D testing over many years, and my reading of the abundant vitamin D research, informs my opinion that the recently released Endocrine Society recommendations are completely obsolete. And they are dangerous in that they may influence practitioners and policymakers to give poor advice and support regarding vitamin D status that will lead to unnecessary poor health outcomes for many.
Mha Atma S Khalsa, DC
http://drmhaatma.com/
As a patient: Elevating my Vit. D levels has alleviated my symptoms of SAD. It has also helped to make my immune system much more resistant to viral infections, and has helped lessen the damage of osteoporosis from hyperparathyroidism.
As an RN: I have seen significant improvement in the health outcomes of patients whose Vit. D levels have normalized.
Katherine Locke, RN, BSN, post-bacc cert.; MSN
Comments from Other Experts
The Scientists Call to D*action vitamin D recommendations from 2007 have stood the test of time. The recommended levels of between 40-60 ng/ml or 100-150 nmol/L are the optimal levels for health and will provide significant risk reduction for many serious diseases with no toxicity concerns.
The three key factors that support these levels (40-60ng/ml or 100-150 nmol/L) that resonate highly with me are:
1. This is the level where parathyroid hormone production is the lowest and calcium is being absorbed most effectively and used to keep your bones strong and healthy.
2. This is the evolutionary level of vitamin D estimated to be found in our ancestral humans as they migrated out of Africa.
3. This is the level that new mothers need in order to provide their newborn infants with sufficient vitamin D through their breast milk.
Perry Holman
Executive Director, Vitamin D Society
The following figure, by Dr. Sunil Wimalawansa (https://doi.org/10.3390/nu15173842), illustrates the desired physiological range of 25(OH)D, shown as 40-80 ng/mL, that covers 99.7% of disorders.[1,2]
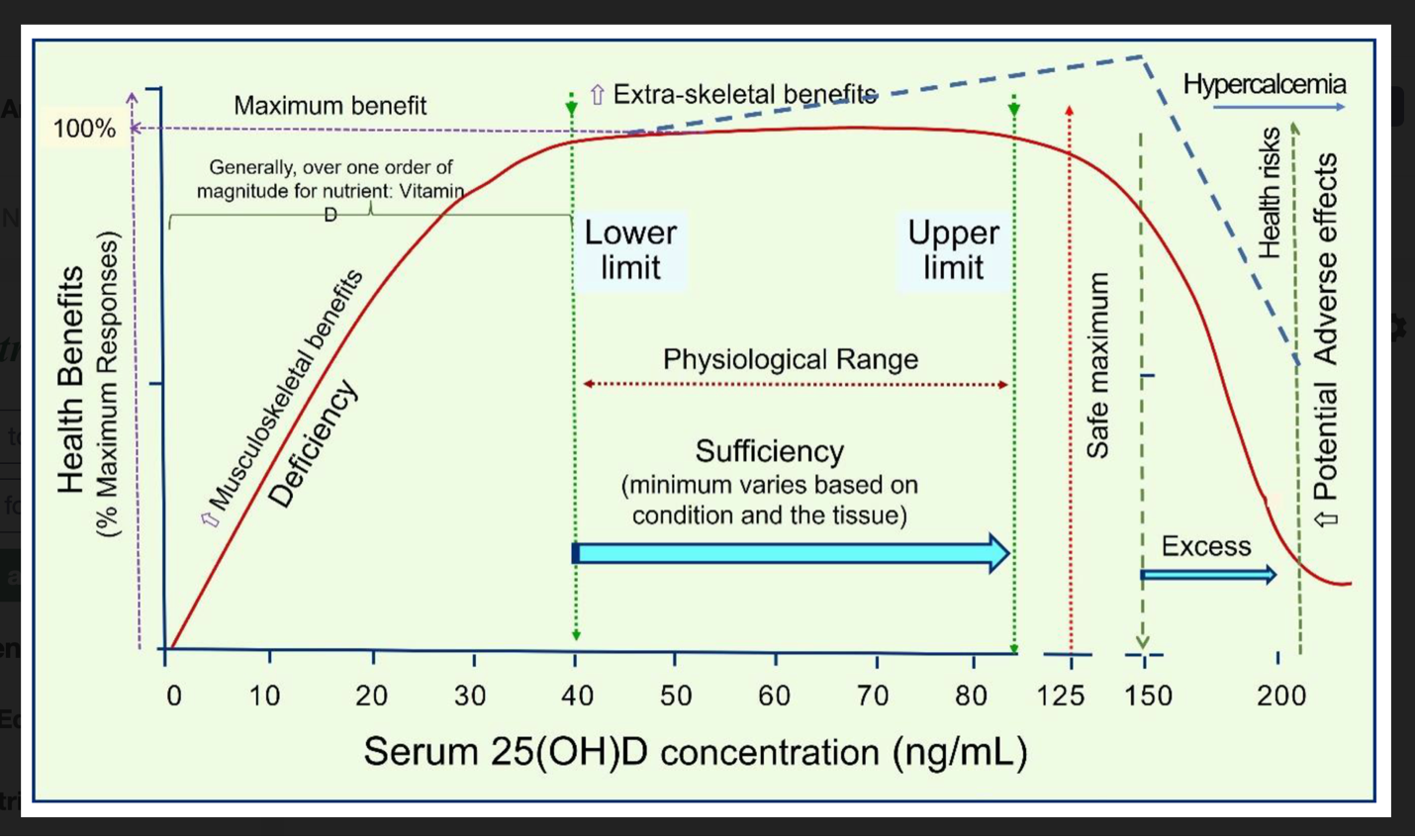
Figure References:
1. Wimalawansa, S. Overcoming infections including COVID-19, by maintaining circulating 25(OH)D concentrations above 50 ng/mL. Pathology & Lab. Medicine Int. 2022, 14, 37–60.
2. Wimalawansa, S.J. Physiological basis for using vitamin D to improve health. Biomedicines 2023, 11, doi:10.3390/biomedicines11061542.
Additional References:
Amon U, Yaguboglu R, Ennis M, Holick MF, Amon J. Safety Data in Patients with Autoimmune Diseases during Treatment with High Doses of Vitamin D3 According to the “Coimbra Protocol”. Nutrients. 2022; 14(8):1575. https://doi.org/10.3390/nu14081575
Dawson-Hughes B, Staten MA, Knowler WC, et al. Intratrial Exposure to Vitamin D and New-Onset Diabetes Among Adults With Prediabetes: A Secondary Analysis From the Vitamin D and Type 2 Diabetes (D2d) Study. Diabetes Care. 2020;43(12):2916-2922. doi:10.2337/dc20-1765
Grant WB, Al Anouti F, Boucher BJ, Dursun E, Gezen-Ak D, Jude EB, Karonova T, Pludowski P. A Narrative Review of the Evidence for Variations in Serum 25-Hydroxyvitamin D Concentration Thresholds for Optimal Health. Nutrients. 2022; 14(3):639. https://doi.org/10.3390/nu14030639
McCullough PJ, Lehrer DS, Amend J. Daily oral dosing of vitamin D3 using 5000 TO 50,000 international units a day in long-term hospitalized patients: Insights from a seven year experience. J Steroid Biochem Mol Biol. 2019;189:228-239. doi:10.1016/j.jsbmb.2018.12.010
McDonnell SL, Baggerly CA, French CB, et al. Breast cancer risk markedly lower with serum 25-hydroxyvitamin D concentrations ≥60 vs <20 ng/ml (150 vs 50 nmol/L): Pooled analysis of two randomized trials and a prospective cohort. PLoS One. 2018;13(6):e0199265. Published 2018 Jun 15. doi:10.1371/journal.pone.0199265
Mirhosseini N, Vatanparast H, Kimball SM. The Association between Serum 25(OH)D Status and Blood Pressure in Participants of a Community-Based Program Taking Vitamin D Supplements. Nutrients. 2017;9(11):1244. Published 2017 Nov 14. doi:10.3390/nu9111244
Shirvani A, Kalajian TA, Song A, Holick MF. Disassociation of Vitamin D’s Calcemic Activity and Non-calcemic Genomic Activity and Individual Responsiveness: A Randomized Controlled Double-Blind Clinical Trial. Sci Rep. 2019;9(1):17685. Published 2019 Nov 27. doi:10.1038/s41598-019-53864-1
Wagner CL, Hulsey TC, Ebeling M, et al. Safety Aspects of a Randomized Clinical Trial of Maternal and Infant Vitamin D Supplementation by Feeding Type Through 7 Months Postpartum. Breastfeed Med. 2020;15(12):765-775. doi:10.1089/bfm.2020.0056
Wimalawansa SJ. Infections and Autoimmunity—The Immune System and Vitamin D: A Systematic Review. Nutrients. 2023; 15(17):3842. https://doi.org/10.3390/nu15173842
Wimalawansa SJ. Non-musculoskeletal benefits of vitamin D. J Steroid Biochem Mol Biol. 2018;175:60-81. doi:10.1016/j.jsbmb.2016.09.016
Wimalawansa SJ. Physiological Basis for Using Vitamin D to Improve Health. Biomedicines. 2023; 11(6):1542. https://doi.org/10.3390/biomedicines11061542